Knowledge Attitude and Practice about Water-Pipe Smoking among Saudi Population ()
1. Introduction
Water-pipe smoking has been popular in Middle Eastern societies for several years, but now becoming more common around the globe [1]. Water-pipe is also known as Shisha, Hookah, Narghile, and Hubble bubble and many other names depending on the country. Many water-pipe smokers have a misconception, which is smoking the water-pipe is less harmful than cigarettes, because the smoke is filtered by the water before it is inhaled [2].
The prevalence of WP smoking was estimated that ranges from 6% to 34% among Middle East countries [3]. Any form of Smoking is a known health hazard being responsible for cardiovascular diseases, lung cancer, chronic bronchitis, and respiratory diseases. In Saudi Arabia, there is a new trend toward increased Shisha smoking [4]. The aim of this study is to measure the knowledge, attitude, and practice of water-pipe (Shisha) smoking among Saudi population and improve the awareness of population.
1.1. Water Pipe
Water-pipe has been used as a social activity in the Middle East and South Asia for more than 400 years [5]. But nowadays the practice has been increasing worldwide in the last few centuries [6]. The prevalence of water-pipe smoking among middle east adult is high [3]. Water-pipe is used to smoking tobacco. Tobacco causes more than 8 million deaths each year. Which is more than 7 million of these deaths is a result of direct tobacco use, while the rest of the deaths are result of non-smokers being exposed to second-hand smoke [6]. The main cause of these deaths is the exposure to smoke toxicants such as tobacco, nicotine, tar, carbon monoxide and heavy metals [7].
Several studies have shown that shisha smoking is practiced more frequently (either daily or once per week). Water pipes are passed from person to person and typical smoking sessions last between 45 and 50 minutes but may continue for several hours [8].
1.2. Toxicological Profile
Even though waterpipe has been present for many years, far fewer studies have examined its chemical constituents/air quality relative to cigarettes. The tobacco is the main source of smoke in both water pipe and cigarettes, water pipe users are exposed to many of the same toxic compounds as cigarette users but at dramatically higher levels, which causes produce worsened health effects in users [9]. Several toxicants have been found in waterpipe smoke including nicotine, carbon monoxide, furanic and phenolic compounds, aldehydes, particulate matter, heavy metals, and ammonia. The amounts of these toxicants may be different in waterpipe compared with cigarette smoke due to different heating process and charcoal combustion [10].
1.3. Nicotine
During an isolated water pipe use session in a clinical research lab, waterpipe smokers have a regular dose of 2.5 mg of nicotine, which was equal to smoking 2 - 3 cigarettes [11]. In normal study of waterpipe smokers in water pipe bars, elevation of urine nicotine concentration around a 73-fold was reported in water pipe smokers after one session [12]. The average plasma nicotine concentration within 24 hours after smoking waterpipe tobacco was equal to smoking 2 to 3 cigarettes [13].
1.4. Carbon Monoxide Poisoning
Carbon monoxide (CO) is an odorless, tasteless, colorless, nonirritating gas formed by hydrocarbon combustion. Carbon monoxide will bind with hemoglobin to form carboxyhemoglobin (COHb) in the blood. The atmospheric concentration of CO is generally below 0.001 percent. CO’s affinity for hemoglobin is more than 243 times greater than that of oxygen [14]. This affinity prevents oxygen from binding to hemoglobin, which leads to hypoxemia and subsequent tissue hypoxia. CO can also precipitate an inflammatory cascade that results in CNS lipid peroxidation and delayed neurologic sequelae [15].
1.5. Health Effects Associated with Water Pipe Smoking
Water-pipe smoking is associated with a variety of adverse health outcomes such as heart disease, cancer, and respiratory illness, these are developed with a long term period. While the short term period adverse health outcome such as Carbon monoxide poisoning. Other adverse health includes the transmission of infectious diseases, such as tuberculosis, owing to the sharing of the water-pipe hose, a common practice in social gatherings [16].
1.6. Effects on the Respiratory System
1.6.1. CO Toxicity
WPS acutely leads to inhalation CO and increased carboxyhemoglobin (COHb) or exhaled CO when compared to cigarette smokers and non-smokers. COHb affects the transportation of oxygen to various organs. CO poisoning can be presented with variable signs and symptoms. These are headache, visual disturbances, vomiting, confusion, ataxia, dyspnea, tachypnea, seizure, ECG changes, dysrhythmias, syncope, retinal hemorrhage, chest pain, bullous skin lesions and focal neurologic deficit [17].
1.6.2. Case Studies and Reports
There were four cases were reported in France, Singapore, and Turkey. The case happens in Saudi Arabia, show the carboxyhemoglobin level (COHb) was 30%, and the case reported in France, shows the carboxyhemoglobin level (COHb) was 20.8%, and Singapore case was 27.8%, and the last two cases in Turkey shows the carboxyhemoglobin level (COHb) was 28.7% and 31.1% [18], There was a case report of CO poisoning in Italy (2011), A female 16 years old smoked tobacco by water pipe for approximately 3 hours, the laboratory analysis of the blood gas, the carboxyhemoglobin level (COHb) was 24% (normal 0% - 1.5%) and which is above the normal range [19].
A study showed average significant decrease in oxygen saturation by 0.39% after a 30 min WPS session [20]. Chronic bronchitis increases the risk of infections and lung cancer; it may also progress to and constitute a part of chronic obstructive pulmonary disease (COPD) [21]. In N. Layoun et al. study, it shows that function of pulmonary and cardiovascular systems was observed to be affected by duration of smoking, age at first WP and quantity of smoking [22]. In M. H. Boskabady et al. study, the water pipe smokers have significantly more wheezing, chest tightness, coughing and sputum production compared with nonsmokers. Also, other studies show water pipe smokers had significantly higher severity and prevalence of respiratory symptoms compared to nonsmokers [23].
1.7. Effects on the Cardiovascular System
High Heart Rate (Tachycardia)
Acute effects of conventional smoking, such as elevated blood pressure, vascular resistance, and heart rate, it’s known for 10 years [24]. In a cohort study, Heart rate elevation that exceeds 50 bpm in 6.4% of participants and reaches more than 200 bpm in 3.6% of participants after 30-min of shisha smoking session [20]. A study showed that changes in the cardiovascular central and peripheral components occur directly after shisha smoking and include high in HR, blood pressure, and after occlusion vascular resistance, while after occlusion blood flow and outflow were reduced [25].
In Selim et al. study, Smokers of both shisha and cigarettes had significantly higher systolic blood pressure and heart rate than exclusively cigarette smokers, shisha smokers, or non-smokers [26]. Acute use of shisha also stimulates changes in the peripheral vascular system in a similar way to cigarette smoking, such that it increased vascular resistance and reduced post occlusion blood flow [27].
In Numair KA et al. study, it was observed after shisha smoking that a mean increase in systolic and diastolic blood pressure and heart rate of shisha smokers. in the same study, they reported that serum concentration of HDL, Apo A in shisha smokers were significantly lower than nonsmokers. However, LDL-cholesterol, Apo B and triglycerides were significantly higher in smokers [28]. Actually, shisha smokers with more than 40 years had three times more risk of having severe stenosis than non-smokers [29]. Shisha smoking was associated with severe coronary artery disease, which was dependent on the duration/frequency of shisha smoking [30].
1.8. Association of WPS with Cancer
In Koul et al. study shows, there was a positive association between the severity of smoking and risk of developing lung cancer [31]. Also in Aoun et al. study, they said the main risk factors of lung cancer among Lebanese women are use of heating fuel and cigarette smoking [32]. Pancreatic cancer is a rapidly fatal disease; it’s associated with tobacco smoking [33]. In Hosseini M et al. study, he reports that shisha smoking is one of the risk factors for prostate cancer [34].
1.9. Infectious Disease
It was rated that the practice of sharing a water-pipe mouth piece shows a serious risk of transmission of communicable diseases including Hepatitis and Tuberculosis [35]. The water pipe and the water inside the Shisha bowl can become an abode to the bacteria such as Mycobacterium tuberculosis; which leads to transmission the TB. It happens when sharing a pipe with someone with pulmonary TB, which leads to a great risk of TB transmission [36].
Studies
In Taha AZ et al. study, it’s shown that the prevalence of shisha smoking among male medical students in Saudi Arabia was 8.6%. A quite similar finding has been reported by Almutairi (2004) who found that among university students in Riyadh 7.3% of the study participants were shisha smokers [37]. In Al-Naggar and Bobryshev study, the finding result about shisha content was 75% of the participants think that shisha contains nicotine, and 79% of the participants think that shisha contains carbon monoxide, 68% of the participants think that shisha contains tar [38]. In Al-Naggar and Bobryshev study, 67.7% of the participants don’t think that water in shisha filtering toxins, while 32.3% of the participants think that water in shisha filtering toxins [38].
In Taha AZ et al. study, it’s shown 70% of participants like to smoking shisha at Cafes or restaurants, while 29% of participants like to smoking shisha at open places, 6% of participants like to smoking shisha at home, 1% of participants like to smoking shisha at sports clubs [37]. In Amin et al. study, it shows 50% of the participants think that Shisha smoking is harmful compared to cigarettes [39].
In Nazeer Khan et al. study when asked about infectious disease transmitted by shisha, 29.8% of the participants choose Tuberculosis, while 18.3% of the participants choose Hepatitis, 11.6% of the participants choose Herpes, 8.5% of the participants choose None [40]. In Amin et al. study, it shows 30% of the participants were smoking shisha every two weeks, 24% smoking shisha weekly, 23% smoking shisha monthly, 21% smoking shisha daily [39].
2. Research Objectives
2.1. General Objectives
To study the Knowledge, attitude and practice about water-pipe (Shisha) smoking among Saudi population.
2.2. Specific Objectives
1) To select the study subjects that include all Saudi males and females who are 18 years old and above.
2) To prepare a self-administered questionnaire that will be composed of End-closed answer that will aim to catch the knowledge of the study subjects regarding the study objective.
3) To publish the questionnaire online to the study subjects by the use of Google Forms and distributing the URL of this questionnaire across multiple multi-media platforms (WhatsApp, Twitter, Telegram, Snapchat and Instagram).
4) To collect the data gathered from the questionnaire in the form of Excel Sheets for each of the study subjects’ answers.
5) To measure the knowledge about water-pipe (Shisha) smoking among Saudi population.
6) To assess attitude towards water-pipe (Shisha) smoking among Saudi population.
7) To evaluate the practice of water-pipe (Shisha) smoking among Saudi population.
8) To estimate the associations between the knowledge, attitude, and the practice about water-pipe (Shisha) Smoking among Saudi population.
3. Methodology
3.1. Study Design
The design of this study was an observational, cross-sectional study on the data obtained from the online self-administered questionnaire about the knowledge, attitude, and practice about water-pipe (Shisha) smoking. Participants of this study were both males and females who are 18 years old and above in Saudi Arabia. The study was conducted from September 2019 to November 2019.
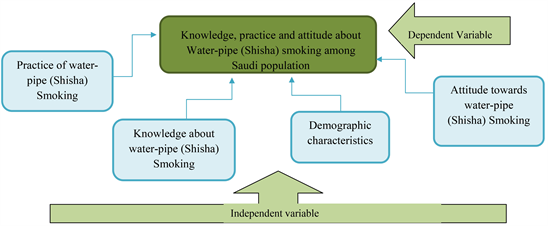
3.2. Conceptual Model of the Study
3.3. Study Sample
This study sample was a group of Saudi males and females who were 18 years old and above. This group of people who were randomly selected with size 1170 people.
3.3.1. Inclusion Criteria
• Saudi female and male participants.
• 18 years old and above participants.
• agreed to participate.
3.3.2. Exclusion Criteria
• non Saudi female and male participants.
• under 18 years old participants.
• declined to participate.
4. Data Collection
Data was collected and obtained by the online questionnaire that has been created in google form and then published in different social media platforms (Twitter, Telegram, WhatsApp, Snapchat and Instagram). Participants filled an Arabic version of the online questionnaire which eased the understanding process for non-English speakers. The questionnaire was divided into 4 parts to cover the aim of the study, one part was for demographic characteristics, another part was for the knowledge about water-pipe (Shisha) smoking, a part for the attitude towards water-pipe (Shisha) smoking, and lastly a part about the practice of water-pipe (Shisha) smoking. Along with an informed consent and an explanation about the study objectives, the participants answered some end-closed MCQs, Multiple Choice Questions, in the span of 10 - 15 minutes.
Data Analysis Plan
Collected data will be entered in Microsoft Excel 2016 and then analyzed by EPI INFO 7 to get descriptive statistics with mean, proportion, percent and frequency distribution. The results will be interpreted in Microsoft Word 2016 in the form of tables and graphs.
5. Ethical Considerations
Ethical approval for this study will be obtained from the Department Research Review Committee, at the College of Applied Medical Sciences at Qaseem University. An informed consent will be given to the participants before they fill the questionnaire, as well as providing an explanation with the study objectives. All the data collected in this study will be kept confidential and used for research purposes only.
6. Results
From Table 1, the highest participants regarding the age criteria were in 18 - 25 years old (83%), and there were more females (70%), while university students were the most in education criteria (43%), and people who have < 5000 SAR income were the most (75%), and there were more people from middle region (Qassim & Riyadh) with percentage (43%).
As Figure 1 shows, 77% of participants that not smoking waterpipe, while 15% smoking waterpipe, 8% were smoking in the previous.
As Figure 2 shows, 81% of participants that smoking waterpipe daily, while 32 % smoking monthly, 26% were smoking weekly.
As Figure 3 shows, 39% of participants that most like to smoking at Shisha bar (café), while 29% like smoking at Home, 29% like to smoking at Other places, 3% like to smoking at Restaurants.
Figure 4 depicts that most, 58% of participants don’t believe that shisha is less
![]()
Table 1. Description of demographic characteristics of the study sample.
![]()
Figure 1. Description of smoking waterpipe.
![]()
Figure 2. Description of the frequency of smoking waterpipe.
![]()
Figure 3. Description of places for smoking waterpipe.
![]()
Figure 4. Description of knowledge about that shisha is less harmful than cigarettes.
harmful than cigarettes, and 20% believe that shisha is less harmful than cigarettes, while 22% didn’t know.
The chart in Figure 5 shows that the most, 78% of participant didn’t know about carbon monoxide poisoning, while 22% know about it.
As a bar chart in Figure 6 shows that 43% of participants didn’t know about the shisha contains. While 38% of participants think that contain all, 8% of them think that only contain nicotine. 6% think it only contains tobacco, while 5% think that contain carbon monoxide.
As pie chart in Figure 7 shows that the most, 54% of participant didn’t know about infectious disease transmitted by shisha, while 27% choose hepatitis, and 13% choose tuberculosis, 6% choose herpes.
The chart in Figure 8 shows that the most, 68% of participant think that water not filter the toxin, while 31% didn’t know, 1% think that water filter the toxin.
7. Discussion
In Taha et al. study, it’s shown that the prevalence of shisha smoking among male medical students in Saudi Arabia was 8.6%. A quite similar finding has been reported by Almutairi (2004) who found that among university students in
![]()
Figure 5. Description of knowledge about carbon monoxide poisoning.
![]()
Figure 6. Description of knowledge about shisha contents.
![]()
Figure 7. Description of knowledge about infectious diseases transmitted by shisha.
Riyadh 7.3% of the study participants were shisha smokers [37]. In our study, we found the total prevalence of shisha smoking was about 15%, with 26% male and 9.6% female, which can be considered as relatively high when compared with Taha and Almutairi studies.
![]()
Figure 8. Description of shisha water effect on toxin.
In Attia Z. Taha, et al. study, it’s shown 70% of participants like to smoking shisha at Cafes or restaurants, while 29% of participants like to smoking shisha at open places, 6% of participants like to smoking shisha at home, 1% of participants like to smoking shisha at sports clubs [37]. This result was similar to our study, 39% of participants like to smoking shisha at shisha bar (Cafes), while 29% of participants like to smoking shisha at home, 29% of participants like to smoking shisha at other places, and 3% like to smoking shisha at restaurants.
In Al-Naggar and Bobryshev study, the finding result about knowledge shisha content was 34% of the participants think that shisha contains nicotine, and 36% of the participants think that shisha contains carbon monoxide, 30% of the participants think that shisha contains tar [38]. In our study shown, 43% of the participants didn’t know about the shisha content, while 38% choose that shisha contains all of tobacco, nicotine and CO, 8% choose only nicotine, 6% choose only tobacco, 5% choose only CO. Unfortunately, most of the participants show a poor knowledge.
In Al-Naggar and Bobryshev study, 67.7% of the participants don’t think that water in shisha filtering toxins, while 32.3% of the participants think that water in shisha filtering toxins [38]. We agree with Al-Naggar and Bobryshev study, 68% of the participants don’t think that water in shisha filtering toxins, while 31% of the participants didn’t know, 1% of the participants think that water in shisha filtering toxins. Which fortunately is considered as good knowledge of the participants.
In Amin et al. study, it shows 50% of the participants think that Shisha smoking is harmful compared to cigarettes [39]. According to our study, 58% of the participants think it’s not less dangerous cigarettes, while 20% of the participants think it’s less dangerous than cigarettes, 22% of the participants didn’t know.
In Amin et al. study, it shows 30% of the participants were smoking shisha every two weeks, 24% smoking shisha weekly, 23% smoking shisha monthly, 21% smoking shisha daily [39]. In this study, it shows 81% of the participants was smoking shisha daily, while 26% was smoking shisha monthly, 32% smoking shisha weekly.
In Nazeer Khan et al. study, when asked about infectious disease transmitted by shisha, 29.8% of the participants choose Tuberculosis, while 18.3% of the participants choose Hepatitis, 11.6% of the participants choose Herpes, 8.5% of the participants choose None [40]. In this study shown, 54% of participant didn’t know about infectious disease transmitted by shisha, while 27% choose hepatitis, and 13% choose tuberculosis, 6% choose herpes. Unfortunately, all the participants show poor knowledge regarding about infectious disease transmitted by shisha.
Many cases were reported about Carbon monoxide poisoning from waterpipe smoking: the first case was reported in Saudi Arabian in 2000, France, Singapore, Turkey and Italy (2011) [18]. Based on these cases we asked our participants about the knowledge of Carbon monoxide poising and we found 78% of the participants show poor knowledge.
8. Conclusion
Most of the study samples were females (18 to 25 years old) university students from the middle region. Our study shows the prevalence of shisha smoking on our participants was low. The misconception that waterpipe is less harmful than cigarettes was not found in this study. More than 39% of waterpipe smokers used shisha bar (café) for smoking. However, they lacked comprehensive knowledge about the shisha contents and carbon monoxide poisoning. Also, they have poor knowledge about the infectious disease transmitted by waterpipe (shisha).
Recommendations
1) Future research should include large and varied sample populations about water pipe smoking.
2) Research studies could focus on carbon monoxide poisoning by water pipe smoking.