Obstructive Hydrocephalus Caused by Pituitary Adenoma: A Case Report ()
1. Introduction
Sellar tumours have a large histological variability and represent approximately 10% - 15% of all intracranial neoplasms; from them pituitary adenomas represent 95% of lesions [1] . Depending on the population surveyed, their reported annual incidence varies from 1.0 to 7.6 per 100,000 populations [2] [3] . Among pituitary tumors, prolactin (PRL)-secreting pituitary adenomas are by far the most frequent ones. Patients with prolactinoma usually present with endocrinological symptoms and, less commonly, with visual defects due to compression of the optic chiasm [4] . The development of symptomatic hydrocephalus due to a pituitary adenoma is an exceptional event. Transnasal surgery for transsphenoidal access to the pituitary and adjacent skull base has undergone rapid evolution in recent years. Surgical approaches through the nose without sublabial incisions have become the norm in many centers throughout the world [5] -[7] . However, the transsphenoidal approach for pituitary adenomas may be complicated by incomplete resection because of limited visualization and inability to maintain free circulation of cerebrospinal fluid [8] . In this report, we describe a patient who had a pituitary adenoma associated with obstructive hydrocephalus treated by endoscopic transnasal transsphenoidal surgery.
2. Case Report
A 37-year-old man presented to us with hairless, headache and visual disturbance in both eyes for three months. Physical examination showed bitemporal hemianopsia. Computerized tomography (CT) scan showed a tumor situated in third ventricle near to the foramen of Monro (Figure 1, Figure 2). A colloid cyst of the third ventricle was initially diagnosed in the patient. Subsequent magnetic resonance imaging (MRI) demonstrated a pituitary macroadenoma (38 × 23 × 21 mm) located mainly outside the sella turcica with suprasellar extension and there was hydrocephalus on the left side of the third ventricle (Figure 3).
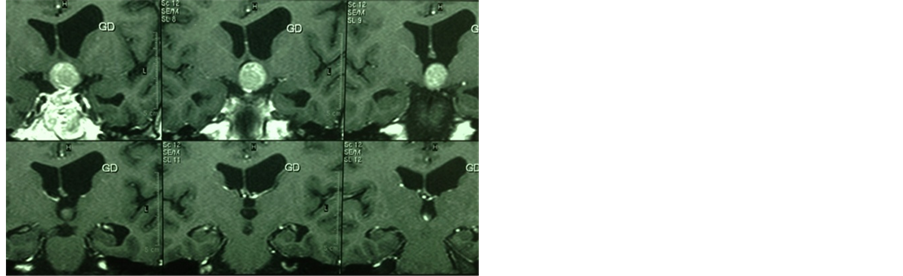
We received the laboratory report that showed a clearly elevated PRL level of 1600 IU/mL (normal level 86 - 324), thus establishing the diagnosis of macroprolactinoma. Low level of testosterone 0.2 ng/mL (normal level 2.49 - 8.36) and high levels of LH 13.9 mU/mL (normal level 1.7 - 8.6) and FSH30.7 mU/mL (normal level 1.5 - 12.4) were observed. Pathological levels of other hormones were: T4: 9.8 mcg/mL (normal level 5.1 - 14), TSH: 1.12 IU/mL (normal level 0.27 - 4.2), Cortisol: 190 ng/mL (normal level 54.9 - 287.5), GH: 0.03 ng/mL (normal level 0 - 4), ACTH: 35.85 pg/mL (normal level 3.6 - 60.5), IGS1: 132.3 pg/mL (normal level 88.3 - 209.9). In a first stage the acutely symptomatic obstructive hydrocephalus was treated with endoscopic transnasal transsphenoidal approach. But there was still a residual tumor mass, which could not be removed by this treatment. Postoperative CT and MRI scans showed resolution of the obstructive hydrocephalus and the foramen of Monro was open (Figures 4-6). Postoperatively, the patient had visual and headache improvement. Subsequently, the patient is a candidate for cranial surgery or medical therapy to complete the treatment.
3. Discussion
The present case was unusual because the patient had a pituitary macroadenoma secreting prolactin with ob-

Figure 1. CT image showing a mass in the foramina of Monro regionthat based on a colloid cyst of the third ventricle is initially diagnosed.

Figure 2. CT image clearly shows hydrocephalus toward the left.
 (a)
(a)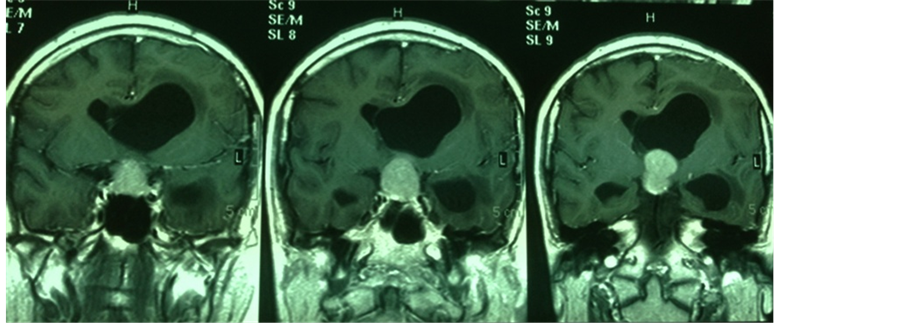 (b)
(b) (c)
(c)
Figure 3. Axial (a), coronal (b) and sagittal (c) MRI images showinga isointense lesion in the suprasellar region with pressure effect on thethird ventricle. Hydrocephalusis seen.
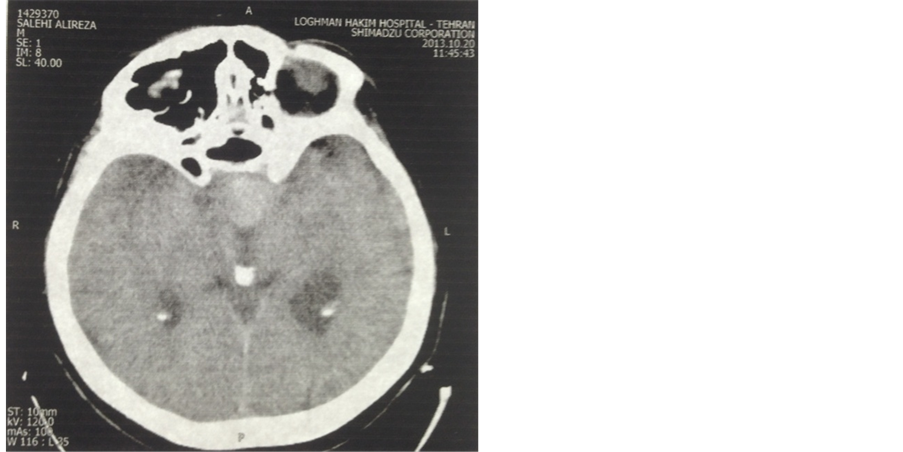
Figure 4. Postoperative CT image showing residual pituitary mass in the suprasellar region.
structive hydrocephalus. Clinical presentation of a pituitary macroadenoma with obstructive hydrocephalus is extremely rare [8] . Therapy of PRL-secreting adenomas is circumscribed to medical therapy with dopamine agonists and surgery, whereas radiation therapy is recommended to the few patients not controlled by both medical and surgical treatments [9] [10] . However, some drawbacks of medical therapy, such as the need for life-long treatment in the majority of patients, side effects limiting compliance by the patient, and resistance of the tumor to dopamine agonists, are still of concern. In recent years, there has been a renewed interest in the surgical treatment of PRL-secreting tumors [11] . Surgery for large-to-giant pituitary adenomas is technically challenging. Usually, microsurgical treatment is recommended for most pituitary adenomas using a transsphenoidal approach [8] . The goals of surgery are to remove the tumor, relieve the mass effect, improve visual abnormalities, reduce hormone hypersecretion to normal levels, and preserve normal pituitary function [1] [12] . Although the transsphenoidal approach has been widely adopted as a safe and effective method for the removal of the majority of pituitary adenomas, large lesions may still present with considerable difficulties [13] -[15] . However, complete resection of tumors with excessive suprasellar extension may be difficult to achieve [8] . The present case highlights the fact that pituitary adenomas with obstructive hydrocephalus should be distinguished from other tumors especially colloid cysts as the prognosis and management with selection of the surgical ap-

Figure 5. Postoperative CT image shows that hydrocephalus has resolved.
 (a)
(a) (b)
(b) (c)
(c)
Figure 6. Axial (a), coronal (b) and sagittal (c) postoperative MRI imagesshowing residual pituitary mass. Hydrocephalus has resolved and theforamen of Monro is open.
proach differs significantly depending on the nature of the lesion. Therefore, the first step of microsurgical treatment (transnasal transsphenoidal approach) was to remove the tumor extending into third ventricle, to resolution of obstructive hydrocephalus. Subsequently, completing the residual tumor resection from suprasellar region will be removed by cranial surgery or the patient will be treated by medical therapy.
NOTES
*Corresponding author.