Large renal carbuncle mimicking intra-abdominal neoplasm on Ga-67 scintigraphy: A case of fever of unknown origin ()
1. INTRODUCTION
Fever of unknown origin (FUO) remains to be a medical challenge despite nowadays technical improvements. It has evolved with time and now has covered wider diagnostic entities including HIV-associated FUO, neutropenic FUO and nosocomial FUO [1]. The diagnosis is made if three outpatient visits or 3 days in the hospital without elucidation of a cause or 1 week of intelligent and invasive ambulatory investigation [1,2]. Despite subsequent evaluations by many tools, up to 50% of cases with FUO reach no final diagnosis [2]. Literatures have indicated that various nuclear medicine images play an important role in investigating FUO [3], among these diagnostic images, 67Ga scintigraphy is a valuable examination and is still used widely [4]. This is because that both inflammatory disorders and some neoplasms can be detected by 67Ga scintigraphy and FUO may be caused by various malignancies. However, this may also tell us that we may not be able to differentiate inflammation from neoplasm on 67Ga scintigraphy. We reported a case with FUO underwent 67Ga scintigraphy with 67Ga avid renal carbuncle mimicking an intra-abdominal neoplasm.
2. CASE REPORT
A 51-year-old man complained of fever for 3 weeks despite out-patient investigations. The cerebrospinal fluid analysis, chest films and abdominal ultrasonography showed negative results. A serum C-reactive protein was 13.86 mg/dL. 67Ga whole body scintigraphy was arranged and the images were taken 65 hours after 6.1 mCi (225.7 MBq) intravenous 67Ga citrate. The planar image revealed dense 67Ga accumulation in left upper abdomen (Figure 1(a)) and the single photon emission computed tomography/computed tomography (SPECT/ CT) revealed that the radiotracers were located at a tumor (Figures 1(b) and (c)). It was unable to differentiate whether it was renal origin or not. Subsequent abdominal contrast-enhanced computed tomography (CT) revealed that the 67Ga avid tumor was a renal cyst (Figures 2(a) and (b)) and a renal calculus was also noticed in the cyst. Previous abdominal CT also demonstrated the renal calculus, however, the cyst was smaller. A midstream urine culture yielded Escherichia coli of 7000 colony forming units per mL. The patient received daily intravenous ceftriaxone 2000 mg and he defeverized after the antibiotic treatment.
3. DISCUSSION
67Ga scintigraphy is a common clinical strategy for pa-
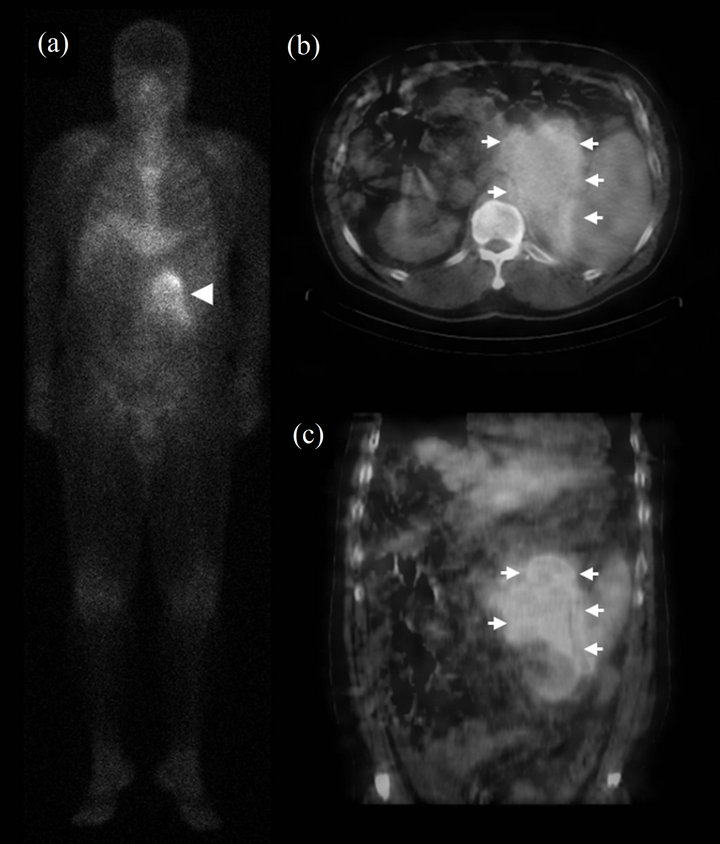
Figure 1. 67Ga whole body scintigraphy: Planar image (a) revealed dense heterogeneous 67Ga accumulation in left upper abdomen (Arrowhead). The trans-axial (b) and coronal (c) SPECT/CT images demonstrated that the 67Ga avid lesion was located at a tumor above or at left kidney (Arrow).
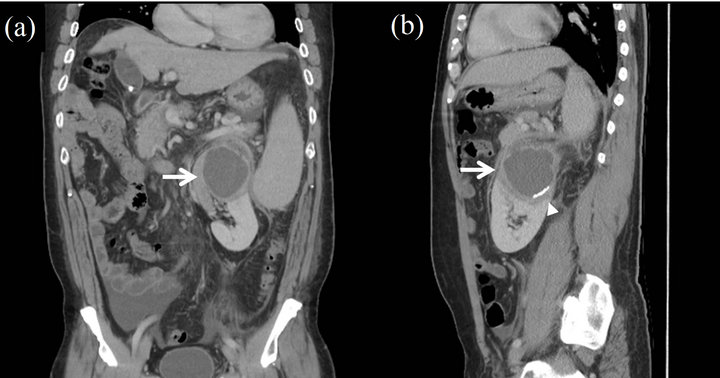
Figure 2. The contrast enhanced computed tomography in coronal section (a) and sagittal section (b) showed a large renal cyst measured to be 7 × 6 cm (Arrow) at upper pole of left kidney, there were many small cystic lesions in the capsule. There was a nephrolithiasis (Arrowhead) in the sagittal section.
tients with FUO. 67Ga behaves like iron and can bind to lactoferrin and siderophore, molecules present at site of inflammation and many neoplasms. According to the literature, 67Ga scintigraphy can be helpful in diagnostic evaluation in 29% of cases with FUO [4]. Among the patients reach final diagnosis from 67Ga scintigraphy, mostly (54%) are infectious, followed by neoplasm (19%) and inflammatory or rheumatologic (16%) [5]. Modern use of integrated SPECT/CT can significantly improve 26% of scan interpretation compared to planar image or SPECT image along [6]. Evidence also suggested that the application of SPECT/CT on 67Ga scintigraphy can further improve diagnosis, localization and definition of extent of disease [7]. In our patient, SPECT/CT localized the lesion successfully; however, the images provided insufficient information to determine the nature of tumor. Further contrast-enhanced CT gave more detailed tissue vascularity information and the final diagnosis was made. Although the integration of CT into SPECT provides anatomical information to functional 67Ga images, noncontrast enhanced CT lakes the information of vascularrity, which is important in differentiating different type of tissues. Thus, with addition of contrast enhanced CT or even performing SPECT/CT with contrast enhancement may further improve the diagnostic performance of FUO.