
1. Introduction
The Early Maladaptive Schema was defined by Jeffrey Young as “a broad pervasive theme or pattern regarding oneself and one’s relationship with others, developed during childhood and elaborated throughout one’s lifetime, and dysfunctional to a significant degree” (Schema Therapy, n.d.). Schemas are patterns which when they are triggered make the person feel intense emotions. This includes memories, physical sensations and cognition (Schema Therapy, n.d.). For example, when the patient has Early Maladaptive Schema, such as abandonment as he has early abandonment memories, he may then feel depressed or may suffer from anxiety, which are related to his early experience of abandonment. As the early maladaptive schema causes intense emotions when activated, those who have more complex characterological problems have several early maladaptive schemas. These make them at higher risk for emotional disorders (Schema Therapy, n.d.).
The schema focused therapy therefore offers a model for treatment for wide range of problems. The schema therapy was developed to address the self defeating patterns, the early maladaptive schemas, which can be lifelong problems. For more than a decade, Young and his associates identified 18 maladaptive schemas. The origins of these schemas are early childhood experiences, the personal temperament of the child and the influence of culture on the child. According to Young’s theory, a combination of the three can cause early maladaptive schemas (Schema Therapy, n.d.).
According to Young, there are types of early childhood experiences that can cause a child to have schemas. These are the following:
• The child who does not get his/her core needs met. The child needed affection, empathy and guidance but didn’t get it etc.
• The child who is traumatized or victimized by a very domineering, abusive or highly critical parent.
• The child who learns primarily by internalizing the parent’s voice. Every child internalizes or identifies with both parents and absorbs certain characteristics of both parents, so when the child internalizes the punitive punishing voice of the parent and absorbs the characteristics they become schemas.
• The child who receives too much of a good thing. The child who is overprotected, overindulged or given an excessive degree of freedom and autonomy without any limits being set (Schema Therapy, n.d.).
In accordance with Young, there are eighteen Early Maladaptive Schemas. These are the unconditional assumptions that the person has about himself and others. Young assumes they are developed during childhood and become life-long assumptions. There are five domains or themes in which the 18 schemas fall under.
The first domain is disconnection and rejection which includes the following schemas: mistrust/abuse, abandonment/instability, defectiveness/shame and social isolation/alienation. These are results of abusive or traumatic childhood experiences. The child usually comes from an unstable family (Beckley, 2007).
The second domain is impaired autonomy and performance, which includes dependence or incompetence, vulnerability to harm, enmeshment and failure. Impaired autonomy and performance is a result of over-protectiveness or neglect of the parents which results in the child feeling incompetent or dependent (Beckley, 2007).
The third domain is impaired limits, which includes entitlement and insufficient self control/self discipline. In this, the internal self control of the child was not developed because the family sets no boundaries on children. As the child did not have rules he then feels a sense of entitlement, and/or will not develop self control (Beckley, 2007).
The fourth is other directedness which includes subjugation, self-sacrifice and approval seeking or recognition seeking. In this, the child experiences conditional love or that the family is concerned with self image. The parents may also be too involved with themselves that the child then continuously seeks approval and recognition (Beckley, 2007).
The fifth is over-vigilance and inhibition, which includes negativity, emotional inhibition, unrelenting standards/hypocriticalness and punitiveness. Here the parents are strict and controlling. The child then becomes emotionally inhibited, pessimistic and extremely critical (Beckley, 2007).
Young and coworkers developed the Young Schema Questionnaire as a self report measure of EMSs (add reference). Various versions were developed and investigated. We will now briefly discuss them and show a related research.
2. Young Schema Inventory 3rd Version/The Young Schema Questionnaire
The Long Form of the Young Schema Inventory, third version (YSQ-L3) is a 232-inventory questions that intend to measure the 18 schemas. The questions require respondents to rate statements that are intended to describe or not describe them. It uses the Likert-type of ranking, specifically, 1 means “completely untrue of me” while 6 means “describes me perfectly” (Dobson, 2009).
Questions range from life experiences, such as, “Most of the time, I haven’t had someone to nurture me, share him/herself with me, or care deeply about everything that happens to me,” to present actions for particular situations, such as, “Often I allow myself to carry through on impulses and express emotions that get me into trouble or hurt other people,” (Young, 2003a). The questions were designed to fully capture the 18 schemas. The cut off values were designed to evaluate each of the schemas as low, medium, high and very high (Dobson, 2009).
The short form of the Young Schema Questionnaire, third edition was also developed, called the YSQ-S3 or the Young Schema Questionnaire: Short Form. Similar with the longer version, the short form uses a Likert-type ranking, whereby 1 means “completely untrue of me” and 6 means “describes me perfectly”. Similarly, questions range from life experiences, such as “For the most part, I have not had someone who really listens to me, understands me, or is tuned into my true needs and feelings,” to present feelings about certain situations, “I feel that I have no choice but to give in to other people’s wishes, or else they will retaliate or reject me in some way,” (Young, 2003b). The YSQ-S3 has been translated to several languages, including German, French, Italian, Portuguese, Korean, Norwegian, Japanese, Turkish, Finnish and Dutch (Dobson, 2009).
However, when it comes to the psychometric properties of the YSQ-S3, several contradicting results have been offered by those who have studied the inventory.
2.1. Results on Reliability of Subscales
A study conducted by Schmidt, Joiner, Young and Telch in 1995 found that the subscales had high test-retest reliability and internal consistency (Dobson, 2009). As for the subscales and specific groups of people who suffer from specific conditions or had similar life events, such as early childhood trauma, the study by Cecero, Nelson and Gilles found strong correlation.
Now, in terms of internal consistency, the study by Wellburn, Corsitine, Dagg, Pontefract and Jordan in 2002 found that the YSQ-S3 showed strong internal consistency. Similarly their study found solid construct validity when tested.
For both the long and short version of the YSQ-S3, it has been found that they have strong internal consistency. Similarly, both versions have demonstrated strong reliability and validity. In fact, the short version can be used in both clinical and non clinical setting. In both settings, the YSQ-S3 long and short versions can be used with generally accurate results (Dobson, 2009).
When it comes to specific disorder, the study by Walter, Mayer and Ohanian evaluated the psychometric properties of both the long and short versions of the YSQ on bulimic women. The study was designed to investigate whether both the long and the short versions of the YSQ have similar psychometric properties, considering that the shorter version lacks in psychometric validation. The study found that both versions demonstrated similar internal consistencies. Moreover, both have the same level of reliability and validity. Although both the long and the short versions of the YSQ showed strong reliability, validity and consistency, the researchers noted that when the test was conducted on bulimic patients and on other groups, further studies were required (Walter et al., 2001).
2.2. Validity of YSQ-S3
In terms of validity in psychological distress, by Schmidt, Joiner, Young and Telch the inventory has shown good overall validity and discriminant validity. Similarly, when it comes to self esteem and susceptibility to depression. The same was demonstrated in symptoms of personality disorder. Schmidt, Joiner, Young and Telch found that a factor analysis confirmed the hypothesized structure of the YSQ-S3. The same is demonstrated in non-clinical populations (Dobson, 2009). Another study conducted by Lee, Taylor and Dunn in 1994 also showed that the test is a good measurement of the schemas. This study was conducted on Australian population and used similar factor analysis. The study used 15 schemas offered in the original inventory.
Another study was conducted on the reliability, validity and consistency of both the short and long version of the YSQ in predicting depression and anxiety. The study found that the short version demonstrated predictive validity in both the depressive symptoms as well as in the depression, using Beck’s Depression Inventory. The shorter version also demonstrated acceptable reliability. In terms of correlation, the study found that the YSQ-subscales are not highly correlated with the YSQ-SF3, contrary to what was expected by the researcher. For example, two of the domains, the negativity/pessimism and emotional inhibition were more correlated with domains one and two. Emotional inhibition on the other hand was more strongly correlated with domains one and four. When it comes to negative live events, EMS have been found to be significantly and strongly correlated with negative life events (Anmuth, 2011).
3. Schema Mode Inventory 2nd Version/Schema Mode Inventory
The Schema Mode Inventory 2nd version is similar to the Young Schema Inventory, third version (YSQ-L3) in the sense that it uses the Likert-type of ranking. Specifically, 1 means “never or almost never”, while 6 means “almost all of the time/always” (Dobson, 2009: p. 333). Respondents are asked to rate statements, such as motivations and actions. For example, “I am trying to do my best at everything I try,” (Dobson, 2009, p. 333).
The SMI was constructed on the basis of longer instruments, by selecting the best items. These were the items for specific modes that do not overlap with the other mode subscales (Schema Therapy, n.d.). The SMI consists of the following scales: vulnerable child, angry child, enraged child, impulsive child, undisciplined child, happy child, compliant surrender, detached protector, detached self-soother, self aggrandizer, bully and attack mode, punitive parent, demanding parent and health adult. The SMI contains 118 items for these categories.
Several studies have proven that the SMI demonstrates strong correlation with the different personality disorders and psychiatric disorders. Moreover, several studies have in fact demonstrated the reliability and validity of the SMI, long and short, across the population and across the different disorders.
3.1. The SMI Reliability
In the study conducted by Arntz, Klokman and Sieswerda on version precursor of the SMI, it was found that participants with borderline personality disorder are more likely to have higher scores on four specific modes. These are on Abandoned Child mode, Detached Protector mode, Angry Child mode and Punitive Parent mode. This study was based on the hypothesis that borderline personality disorder is a result of one of four maladaptive schema modes. This was the first empirical study on the model. It investigated whether the four identified modes are indeed specific to the borderline personality disorder, specifically the Detached Protector, the Punitive Parent, the Abused/Abandoned Child and the Angry/Impulsive Child (Arntz et al., 2005).
The study also investigated whether the stress of the individual with borderline personality disorder would increase the detached protector mode of the schema. To investigate, the subjects who have borderline personality disorder were tested using the SMI and then they were asked to watch borderline personality disorder-specific movie fragments. Later on they were asked again to answer the SMI. The study found that the borderline personality disorder patients were characterized by four maladaptive modes, specifically the Detached Protector, Punitive Parent, Abused/Abandoned Child, Angry/Impulsive Child, which were originally hypothesized by the study. Moreover, the study found that borderline personality disorder patients scored lowest in the Healthy Adult Mode. This study proved a strong correlation between the SMI and borderline personality disorder (Arntz et al., 2005).
When it comes to the correlation among the different modes with the different personality disorders, the study by Lobbestael, Van Vreeswijk and Arntz found that there are patterns on the modes for those with the disorders. The pattern varies according to the disorder but all in all for the personality disorder, it shows significant pattern, demonstrating specific disorder. This proves a strong correlation between the SMI modes as assessed with personality disorders. In this study, the researchers assessed 489 patients under the axis I, axis II and non patients (Lobbestael et al., 2008).
To assess the relationship between the fourteen schema modes as they apply to individuals with personality disorders, the individuals were assessed psychopathologically with the Structured Clinical Interview for DSM-IV axis I and axis II disorders (SCID I and SCID II) or the Structural Interview for DSM-IV Personality Disorders (SIDP-IV). At the same time, it must be noted that although several studies have been proven to be quite consistent in terms of validity and reliability of the SMI for people with personality disorders, people with psychiatric disorders and healthy people, there could be a problem for certain population in terms of self-rating. Those who have different perceptions about themselves and others for example may answer the questions inaccurately.
This has in fact been proven to be quite true in a study conducted on patients with antisocial borderline or cluster C personality disorders. The study investigated whether the Schema Mode Inventory, as it is self reported by patients, would be consistent with the reports of the therapist. The study made use of 92 patients with the said disorders. When the results were compared, there was significant discrepancy between the report of the therapist and the patients with antisocial personality disorder. The discrepancy was significant when compared to the results of the patients with borderline personality disorder and cluster C patients. The patients with antisocial personality disorder demonstrated less maladaptive modes. But with the adaptive modes, the report of the therapist is the same as their self report. The researchers suggested that with the antisocial personality disorder a different assessment method is required than the SMI (Lobbestael et al., 2009).
Lastly, a most recent study on the reliability and validity of the Schema Mode Inventory was conducted by Lobbestael, Van Vreeswijk, Spinhoven, Schouten, & Arntz. The study was conducted by first establishing what the items of the short Schema Mode Inventory are. Following this, the study assessed the psychometric properties of the short Schema Mode Inventory. In assessing the psychometric properties, the study tested the factor structure, internal reliability and test retest reliability. At the same time, the study tested the correlations of the subscale and the monotonical increase of the modes. In order to test all these, the study used both health patient and patients with disorders. The study found that the short Schema Mode Inventory have good internal consistency on the subscales. The study also found that it had moderate construct. When it comes to the test retest reliability, the SMI demonstrated good test retest reliability, similar with its internal consistency. Moreover, the test has been proven to be consistent in predicting some of the Axis II pathology. At the same time, some of the modes are accurate in predicting the severity of the disorders in Axis I and Axis II (Lobbestael et al., 2010).
3.2. The SMI Validity
When it comes to validity, SMI shows strong construct validity when tested and evaluated. However, as there is a significant correlation between the personality disorders and the modes, some studies suggest that there is a need for a more specific mode or modes that corresponds specifically with the personality disorders (Dobson, 2009).
In terms of specific personality disorders, the study by Bamelis, Renner, Heidkamp and Arntz found that the SMI is a very useful tool in clinical practice, alongside the Schema therapy. In the study, the researchers investigated cluster-C, paranoid, histrionic and narcissistic personality disorders in relation to the 18 modes of the Schema Mode Inventory. The test has been found to be quite accurate in differentiating those with personality disorders and those who are healthy. Similarly, the SMI mode subscales demonstrated strong correlation with various clinical psychiatric disorders. This was proven by the study on fifty individuals who were tested using the SMI during routine psychological assessment. The researchers concluded that SMI is a good tool for assessment for wide range of psychiatric disorders. Moreover, the researchers, based on this, also concluded that the Schema Focused Therapy may significantly help the patients with psychiatric disorders (Khalily et al., 2011).
Although the SMI has been proven to be effective in identifying personality disorders and psychiatric disorders there was a problem of the schema mode constructs in having a clear scientific and therapeutic guidelines under clinical practice. Thus, although the test demonstrates a strong correlation with the disorders, it is deemed separately from the schema mode therapy. In short, there is a lack of connection that links the test with the schema mode therapy. Although the test has been proven to be quite accurate in predicting the different disorders, even the specific disorders, it was deemed distinct from the schema therapy.
In order to address this problem, a study was conducted to clarify the schema modes theoretically and therapeutically. The study thus identified the various aspects of the individual self that demonstrates the cognition, behavior and emotions that are active in the individual. The schema modes were then presented for these active emotions, cognition and behavior. Second the modes were conceptualized for the different personality disorders. Third, the modes were outlined for those with the healthy individuals and for those with pathological problems. These are under the premise of clinical and scientific guidelines and not mere theoretical assumptions. Lastly, although the researchers indicated that this demonstrates significant progress in the use of the SMI in the schema mode therapy, they suggested that further studies would be even more beneficial (Lobbestael et al., 2007).
3.3. Present Study
The present Study aims to validate the Greek versions of the YSQ-3 and the SMI-2nd version (2009) in a mixed sample of patients with various axis-I and II disorders, and non-patients.
It was expected that the two inventories will have high reliability (assessed by internal consistency estimates), and that a factor analysis will confirm the structure of their original design. Furthermore it is believed that there will be correlations between the YSQ and SMI subscales. Moreover a comparison between a patient and a non-patient for the results of the YSQ and the SMI will be conducted and as well as another MANOVA about the deviation contrasts for the diagnostic groups of the clinical participants. We expected deviant scores on all subscales of both instruments in the patients compared to the non-patients (higher on pathological scales, lower on healthy scales). Lastly, we expected specific disorders to be characterized by specific YSQ and SMI subscales.
4. Method
4.1. Participants
The participants of the present study are 1441 Greek adults, 581 inpatients and 679 outpatients from the Private and Public Psychiatric Hospitals and practitioners, and 181 non-patients. Table 1 gives an overview of the demographics. The inpatients and outpatients were diagnosed with a wide range of disorders from Axis I and II, with diagnoses made by the psychiatrist and clinical psychologists, treating those participants based on the their clinical evaluation and the psychometric results from the Greek Version of the Personality Assessment Inventory. The most common disorders were Depression (11.5%), Borderline PD (7.4%), and Drug Addiction (9.7%) (Table 2). Participants that had not reached the 18th year of age and people who were diagnosed with dementia were excluded.
4.2. Materials
Young Schema Questionnaire (Short version): the YSQ is a self-administered questionnaire consisted by 205 questions, which are answered by the participant on a 6-point Likert scale. The questions are examining all 18 schemas 3).
The Schema Mode Inventory: The SMI was developed by Young et al. in 2008. It consists by 124 questions answered by the participants on a 6-point Likert scale. This questionnaire examined 16 possible SMs.
5. Procedure
At first both inventories were translated in Greek by English Literature teachers, who had the Greek language as their native tongue and then they were back translated in English in order to examine possible discrepancies in the original translations. The only instruction that was given to the teachers was to make sure that they kept the meaning of each statement and that they should syntax the Greek statements simple, in order to be easy to understand. The final version of the two questionnaires in Greek was formed with the questions that in the backtranslation were more accurately to the English questions. Since the language of both questionnaires is simple and easy for the participants to understand, there were no problems in the translation and back-translation.
Clinical participants were invited to participate by the hospitals physicians. The physicians informed briefly the potential participants about the study and asked them whether they would like to participate in a group meeting, where the description of the study and the filling in of the questionnaires took place after a participation form was signed by them. All the participants who signed completed the questionnaires.
The non-patients were sampled by an advertisement posted on a psychologist’s website, inviting them to participate on completing a set of questionnaires. Whoever agreed to participate they completed online the before mentioned questionnaires. The participants had the option to fill in their email address in order to receive a brief report of the results.
Analysis
The statistical analysis consisted of three parts: reliability analysis, factor analysis and investigation of associations between YSQ and SMI subscales.
For the first part internal consistency (Cronbach’s alpha) all the subscales were estimated, and item-rest correlations as well as change in Cronbach alpha if the item would be deleted were inspected, in three subsamples: non-patients, outpatients and inpatients For the second part of the study, confirmatory factor analysis with structural equation modeling for both inventories was conducted, in the whole sample.
Associations between the instruments’ subscales were assessed by calculation of Pearson correlations. Given the 16 × 18 = 288 correlations, critical alpha was set at p = .00017 (Bonferroni correction).
A MANOVA followed up by unvaried group contrasts was used to assess differences between patients and non-patients on the subscales of the instruments.
For testing whether specific subscales characterized specific diagnostic groups, a MANOVA followed up by deviation contrasts was employed with the 15 diagnostic groups with a sample size larger than 14 (Table 2).
6. Results
Reliability analysis. Internal consistencies as estimated by Cronbach alpha are presented in Table 3 for the YSQ and in Table 4for the SMI-2. As can be seen the subscales of both questionnaires had high reliability, Ranging from .85 to .97 (mean = .91) for the YSQ and .64 to .98 (mean = .81) for the SMI. Inspection of individual items did not indicate severe problems, so all items were retained. With the exception of EMS 12 and EMS 13, in no other factor of either questionnaire there was no increase in the alpha if an item was deleted. On both EMS 12 and EMS13 it was decided not to delete those items, since the change would be minimal.
6.1. Factor structure
Factor loadings on the intended factors varied from .55 to .94, mean .74 for the YSQ; and from .64 to .89

Table 3. Crombach’s Alpha for YSQ-3rd.
ED: Emotional Deprivation; AB: Abandonment; MA: Mistrust Abuse; SI: Social Isolation; DS: Defectiveness Shame; FA: Failure to Achieve; DI: Dependence Incompetence; VH: Vulnerability to Harm; EM: Enmeshment; SB: Subjugation; SS: Self-Sacrifice; EI: Emotional Inhibition; US: Unrelenting Standards; ET: Entitlement; IS: Insufficient Self-Control; AS: Approval Seeking; NP: Negativity Pessimism; PU: Punitiveness.
Table 4 . Crombach’s Alpha for SMI.
VC: Vulnerable Child; AC: Angry Child; EC: Enraged Child; IC: Impulsive Child; UC: Undisciplined Child; HC: Happy Child; CS: Compliant Surrender; DP: Detached Protector; SS: Self-Soother; SA: Self-Aggrandizer; BA: Bully and Attack; PP: Punitive Parent; DP: Demanding Parent; HA: Healthy Adult; PO: Perfectionist Overcotroller; SO: Suspicious Overcontroller.
mean .76, for the SMI.
6.2. Associations between the Instruments’ Subscales
From Table 5 it can be seen that there was a number of correlations, both positive and negative, between the subscales of the YSQ and SMI. We will focus on the strongest positive and negative correlations observed for
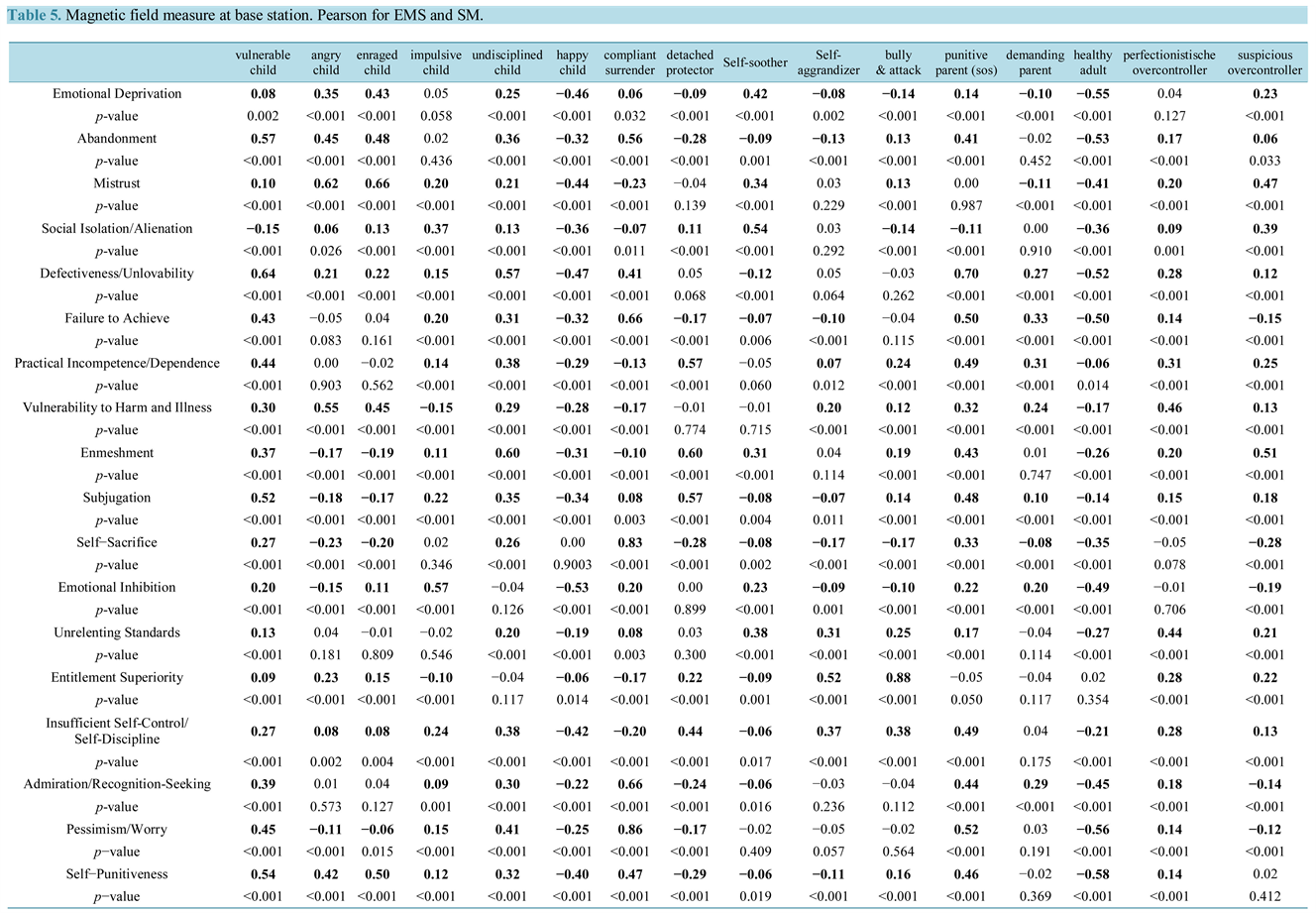
Table 5. Magnetic field measure at base station.Pearson for EMS ans SM.
each EMS:
• The Emotional Deprivation scale is positively associated with the Enraged Child (r = .43 and p-value < .001), and negatively with the Healthy Adult scale (r = −.55 and p-value < .001).
• The Abandonment scale is positively associated with Vulnerable Child (r = 0.57 and p-value < .001), and negatively with the Healthy Adult scale (r = −.53 and p-value < .001).
• The Mistrust scale is positively associated with the Enraged Child (r = .66 and p-value < .001), and negatively d with Happy Child scale (r = −.44 and p-value < .001).
• The Social Isolation scale is positively associated with the Self-Soother (r = .54 and p-value < .001) and negatively with the Happy Child scale (r = −.36 and p-value < .001) and the Healthy Adult scale (r = −.36 and p-value < .001).
• The Defectiveness-Shame scale is positively associated with the Punitive Parent (r = .70 and p-value < .001) and negatively with Healthy Adult scale (r = −.52 and p-value < .001).
• The Failure to Achieve scale is positively associated with Compliant Surrender scale (r = .66 and p-value < .001) and negatively with the Healthy Adult scale(r = −.50 and p-value < .001).
• The Practical Incompetence scale is positively associated with Detached Protector scale (r = .57 and p-value < .001) and negatively with Happy Child scale (r = −.29 and p-value < .001).
• The Vulnerability to Harm and Illness scale is positively associated with the Angry Child scale (r = .55 and p-value < .001) and negatively with the Happy Child scale (r = −.28 and p-value < .001).
• The Enmeshment scale is positively associated with the Undisciplined Child scale (r = .60 and p-value < .001) and the Detached Protector scale (r = .60 and p-value < .001). Furthermore the Enmeshment scale is negatively associated with the Happy Child scalev (r = −.31 and p-value < .001).
• The Subjugation scale is positively associated with the Vulnerable Child scale (r = .52 and p-value < .001) and negatively with the Angry Child scale (r = −.18 and p-value < .001).
• The Self-Sacrifice scale is positively associated with the Compliant Surrender scale (r = .83 and p-value < .001) and negatively with the Healthy Adult scale (r = −.35 and p-value < .001) and the Suspicious Overcontroller scale (r = −.28 and p-value < .001).
• The Emotional Inhibition scale is positively associated the Vulnerable Child scale (r = .22 and p-value < .001), the Punitive Parent scale (r = .22 and p-value < .001) and the Demanding Parent scale (r = .22 and p-value < .001). Furthermore Emotional Inhibition is negatively associated with the Happy Child scale (r = −.53 and p-value < .001).
• The Unrelenting Standards scale is positively associated with the Perfectionistische Overcontroller scale (r = .44 and p-value < .001) and negatively the Healthy Adult scale (r = −.27 and p-value < .001).
• The Entitlement-Superiority scale is positively associated the Bully & Attack scale(r = .88 and p-value < .001) and negatively with the Compliant Surrender scale (r = −.17 and p-value < .001).
• The Insufficient Self-Control scale is positively associated with the Punitive Parent scale (r = .70 and p-value < .001), and negatively with the Happy Child scale (r = −.42 and p-value < .001).
• The Recognition Seeking scale is positively associated with the Compliant Surrender scale (r = .66 and p-value < .001), and negatively with the Detached Protector (r = −.44 and p-value < .001), and the Healthy Adult scales (r = −.45 and p-value < .001).
• The Pessimism scale is positively associated with the Compliant Surrender scale (r = .86 and p-value < .001) and negatively with the Healthy Adult scale (r = −.56 and p-value < .001)
• The Punitiveness scale is positively associated with the Vulnerable Child scale (r = .54 and p-value < .001), and negatively with the Healthy Adult scale(r = −.58 and p-value < .001).
MANOVA analysis between patients and nonpatients. We tested the hypothesis that the GROUP variable (nonpatient = 0, patient = 1) has a significant impact on all YSQ and SMI subscale scores considered as a group. This is done with the General Linear Model/Multivariate procedure in SPSS. A one-way MANOVA revealed a significant multivariate main effect for GROUP, Pillai’s trace = .986, F (34,1395) = 2981,467, p < .001, partial eta squared = .986. Power to detect the effect was very high. Given the significance of the overall test, the univariate main effects were examined. Significant univariate main effects for GROUP were obtained for all YSQ and SMI subscale scores.
The Box’s Test of Equality of Covariance Matrices was significant (p < .001) indicating that the observed covariance matrices of the dependent variables are not equal across groups. This is, in general considered to be a violation of the assumptions of the MANOVA procedure. Nevertheless we can accept the results of the Manova procedure since our sample is large enough (Table 6).
MANOVA between diagnoses. We implemented the General Linear Model/Multivariate procedure in SPSS in order to test the hypothesis that the diagnosis has a significant impact on all YSQ and SMI subscale scores considered as a combined group. We created a new variable DIAGNOSIS which included only those diagnostic groups with sample size > 14. This was the independent variable in our model. All YSQ and SMI subscale scores were the factors (dependent variables). A one-way MANOVA revealed a significant multivariate main effect for DIAGNOSIS, Pillai’s trace = 10,126, F (554,21984) = 69,673, p < .001, partial eta squared = .634. Power to detect the effect was very high.
Given the significance of the overall test, the univariate main effects were examined. Significant univariate main effects for GROUP were obtained for all YSQ and SMI subscale scores (Table 7).
We calculated Cohen’s d effect size of the differences in scores (mean difference divided by the pooled standard deviations Sp ). Presented on tables 8-10.
Table 6 . MANOVA between Patients and Nonpatients.
More specifically we used the formula:
where, μ1, μ2, the means of the 2 groups and  the pooled Std:
the pooled Std:
 is considered to be a small effect size,
is considered to be a small effect size,
 is a moderate effect size, and
is a moderate effect size, and
Table 8. Cohen analysis between no psychopathology and inpatients.
 is a large effect size.
is a large effect size.
7. Discussion
The aim of the present study was to validate the SMI-2nd version and the YSQ 3rd version on the Greek language. For the validation procedure we have followed three steps. First the reliability analysis and the evaluation of the internal consistency, second the factor analysis for each of the inventories as in the studies of Lebbesteal et al. 2010, Young, 2003a and Walter, 2001. The third step was the examination of correlations between the YSQ and SMI subscales. The fourth step was the comparison between the patient-non-patient comparison for the results of the YSQ and the SMI and the fifth step was the MANOVA about the deviation contrasts for the diagnostic groups of the clinical participants.
For the validation of the SMI and YSQ-3rd version, initially we have conducted a translation from English to Greek and back-translation. During the procedure we evaluated the accuracy of the statements on the Greek ver
Table 9. Cohen analysis between no psychopathology and outpatients.
sion of the inventories, which was high in terms of the meaning of the content for each statement.
During the distribution phase for the study there were no problems with either the patient sample or the healthy sample.
7.1. Reliability Analysis
From the reliability analysis presented above, it can be seen that both inventories presented a strong reliability and internal consistency.
7.2. Factor Analysis
As it has been presented on the results, in both questionnaires the factors were confirmed as in the original studies. Specifically all 18 schemas-factors were confirmed for the YSQ and all 16 modes-factors were confirmed
Table 10. Cohen analysis between inpatients and outpatients.
for the SMI. There were not found any questions, in the present analysis that loaded on a different factor that on the original design of the inventories.
7.3. Correlation between EMSs and SMs
On the results section we have outlined the main positive and negative correlation between each EMS with SM.
From the correlational analysis some interesting finding were produced. Specifically on the first section of the EMSs “Disconnection and Rejection”, with the exemption of the Mistrust Abuse schema, all other schemas have a negative correlation with the Healthy Adult Mode. The explanation for that finding is that those schemas describe the need that one has for security, support and guidance, which is in essence what the Healthy Adult mode provides. The Mistrust schema is negatively associated with Happy Child, which can be explained, because mistrust includes the expectation that others will hurt or humiliate the person on purpose. On the other hand Happy Child feels loved and supported, which is the opposite belief, hence the negative correlation (Young, 2003b; Anmuth, 2011).
On the “Impaired Autonomy and Performance” group of the Schemas, again a common factor was found on the negative correlation. Specifically, with the exemption of the Failure schema, all others are negatively associated with Happy Child. That can be explained by the fact that this group describes in essence the perceived ability, or inability to do something and the undermined child confidence, which is exactly the opposite of what the Happy Child Mode describes. The Failure Schema, which, as we have mentioned, is negatively correlated with Happy Adult. This correlation can be explained in the sense of a consequence. The Failure schema describes the belief that one has failed, hence the difficulty of performing adult functions (Young, 2003b; Anmuth, 2011).
On the group of the “Impaired Limits” Schemas again the common factor is the negative correlation of both schemas with the Happy Child. This group describes problems that are mainly associated with the lack of one’s guidance as a child, hence the negative correlation with the happy child mode. Another interesting finding is the negative correlation that was found between Entitlement, the belief that someone is superior to others and that others should comply with ones demands and the Compliant Surrender, the tendency that one gives in to the demands of others in order to avoid pain or rejection (Young, 2003b; Anmuth, 2011).
On schema group “Overvigilance and Inhibition”, all schemas have a negative correlation with the Happy Adult mode. The present group includes schemas that describe the suppression of feelings, impulses and desires, because, among other things, to avoid criticism. The Happy Parent mode, on the other hand, among other things, validates and enforces the “child”, hence the negative correlation that was produced. Furthermore, as it is stated, the families of the people who have schemas form that group are demanding, grim and punitive, the exact opposite of the Happy Adult mode (Young, 2003b; Anmuth, 2011).
On the final group of the schemas, there were not found any commonalities between the correlations found. The Subjugation schema produced a negative correlation between with the Angry Child more. That can be explained based on the fact that the schema describes someone who feels coerced, to avoid anger, while the mode describes a “child” who expresses anger because of perceived injustices and mistreatments. The other schema Self-sacrifice describes the excessive focus of the needs of others at the expense of one’s actual needs. One of the explanations for the present schema is the conditional acceptance of his/her family and it is negative correlated with the Happy Adult mode, which describes the exact opposite, the unconditional acceptance. Finally the Approval-Seeking schema is about the belief that one gives excessive emphasis on gaining approval and recognition from others. This schema is negatively correlated with the Detached Protector mode, which describes one who is emotionally distant, avoids getting close to others and does not pay attention to the other’s opinion (Young, 2003b; Anmuth, 2011).
Finally all positive correlations produced between schemas and modes are similar in terms of beliefs and behaviors.
About the Cohen Analysis conducted. The comparison between the No Psychopathy vs. Outpatient groups (Table 8) of the variable Self-Sacrifice showed a statistical significant mean difference with a relatively small effect size. All other comparisons showed a statistical significant mean difference with a large effect size.
The comparison between the No Psychopathy vs. Inpatient groups (Table 9) of the variable Self-Sacrifice didn’t show a statistical significant mean difference. The effect size was also small. All other comparisons had a statistical significant mean difference with a large effect size.
The comparison between the Inpatient vs. Outpatient groups (Table 10) of the variables emotional inhibition, impulsive child, self-aggrandizer, bully & attack, healthy adult and perfectionistische overcontroller showed a statistical significant mean difference but with a relatively small effect size (close to 0.2). All other comparisons didn’t show a statistical significant mean difference. Their effect size was also small.