Cross-cultural psychometric assessment of the parent-teen sexual risk communication (PTSRC-III) scale in Jamaica ()
1. INTRODUCTION
In the Caribbean, HIV/AIDS rates are high, with only countries in sub-Saharan Africa having higher rates [1]. Adult HIV prevalence in the Caribbean ranges from a low of 0.1% in Cuba to a high of 3.1% in the Bahamas [1]. In Jamaica, the largest English-speaking Caribbean island, the HIV prevalence among adults, 15- to 49-yearold, is estimated to be 1.7% [1]. There are an estimated 32,000 (range 21,000 - 45,000) persons living with HIV/ AIDS in Jamaica. HIV/AIDS rates vary across the island, but are highest in urban areas (e.g., Kingston/St. Andrew and St. Catherine) and coastal tourist areas (St. Ann and St. James). In 2009, 66% of reported HIV/AIDS cases were from these parishes [2].
The primary mode of HIV transmission in Jamaica is heterosexual contact, with more than 90% of adult cases attributed to heterosexual practices [2]. There is a great sex-disparity in HIV prevalence in adolescents and young adults in the Caribbean. HIV prevalence among 15- to 24-year-old females in the Caribbean is twice that of males, 0.8% vs. 0.4%, respectively [1]. These same disparities are seen in Jamaica [2-4].
1.1. HIV/AIDS in Jamaican Adolescent Girls
Jamaican female adolescents face much higher risk for HIV infection compared to male adolescents [3-6]. The cumulative AIDS case rate (per 100,000 population) among 10- to 19-year-olds was more than three times higher in females (62.7) compared to males (19.2) [2]. Several factors have been advanced to explain this elevated HIV/AIDS risk, including early sexual debut, unprotected sexual intercourse, sexual abuse, transactional sex with older men, and multiple sexual partnerships [5, 7-11]. More than half of Jamaican adolescent girls have sex before the age of 15 years [4-5,12-15]. Many adolescent girls engage in sexual relationships with older men in exchange for money or gifts [6,12,13,16,17]. Both early sexual debut and older male partners increase the likelihood of sexually transmitted infections (STIs) as well as HIV and unplanned pregnancy [12,16,18]. Often these girls lack condom use self-efficacy and/or have less power to refuse unsafe sex or negotiate condom use with older partners [6,16].
Sexual coercion and intimate partner violence are also serious issues in Jamaica that may compromise young women’s abilities to refuse sex or negotiate for condom use. Approximately 11.9% of sexually active Jamaicans, 15- to 49-years-old, report they have been coerced or pressured to have sex. The proportion is even higher (13.1%) among adolescent and young adult women, 15- to 24-years-old [16]. Sexual coercion and partner violence are more likely to occur among adolescent girls who are younger than their male sexual partners [4,12, 14,15,17-19].
Jamaican adolescent girls and young women who engage in transactional sex, casual sex and sex with multiple partners use condoms less consistently than others [6,12,14-16]. Further complicating their risk is the lack of perceived risk for HIV and other sexually transmitted infections (STIs). Almost two-thirds of Jamaicans who report having multiple sexual partners and using condoms infrequently believe that they had little or no risk of contracting HIV infection [16].
1.2. Parent Influences of Adolescent Sexual Risk
Interactions between parents/caregivers and their adolescent children have been shown to substantially influence the sexual risk beliefs and behavior of adolescents. US studies have identified a number of important parental influences, including parental monitoring and supervision, high quality parent-teen relationships, parent-teen sexual communication and less permissive parental attitudes towards adolescent sex [20-34]. Of these, parentchild sexual communication has been singled out as being particularly important. Parent-teen sexual communication has been associated with improved adolescent resistance to sexual pressure from peers, delays in sexual initiation, and reduced sexual risk-taking [26-32,35-39]. Unfortunately, there is a dearth of research outside of the US examining family influences of adolescent sexual risk taking. Although a few studies have been undertaken in Europe [40] and Mexico [37,38], no such studies have been conducted in the Caribbean.
1.3. Parental Expansion of the Theory of Planned Behavior
Consistent with the findings in the literature noted above, the Parental Expansion of the Theory of Planned Behavior [35] provides a conceptual framework to guide the study of family influences on adolescent sexual risk. The original Theory of Planned Behavior (TPB) [41] is a widely used model for understanding individuals’ intentions to perform a given behavior. In short, the TPB posits that individuals’ intentions are determined by their attitudes and beliefs toward the behavior, their perceptions of whether important others would approve, and their perceived control over the behavior. The Parental Expansion of the TPB builds upon the original model by explicitly acknowledging that parents are among the most proximal and important influences of adolescents’ sexual risk-related beliefs and, in turn, their intentions and behaviors [35]. In both the TPB and the Parental Expansion of the TPB, there is a recognition that beliefs, intentions and behaviors occur within and are influenced by the larger socio-cultural context. In addition, the relative importance of behavioral beliefs, normative beliefs, and control beliefs may vary from culture to culture. Thus, when using either model to understand behavior or develop behavioral interventions, extensive elicitation research is needed to understand the culture-specific influences operating within a given group [35,42,43]. Culturally sensitive and valid instruments are also needed to assess influential parenting behaviors and other salient influences of adolescent sexual risk behavior.
1.4. The Parent-Teen Sexual Risk Communication Scale
The Parent Teen Sexual Risk Communication Scale (PTSRC) was developed to quantify and measure one of the most important parental influences of adolescent sexual beliefs and behaviors, sexual communication. The scale assesses the amount of informational sexual communication occurring between adolescents and each of their parents or guardians [24]. The most recent version, the PTSRC-III, has undergone extensive psychometric testing and demonstrated a stable two factor structure, reliability and validity when used with various adolescent groups within the US (e.g., college students, late adolescent licensed drivers, adolescent females) [24,31]. In addition, the scale has been employed in studies in Mexico [37,38], and in ongoing studies in South Africa and Jamaica.
However, the cross-cultural validity of instruments may not be assumed. A cross-cultural assessment of the PTSRC-III is important to determine whether the scale is a valid and reliable measure of parent-teen sexual risk communication when used with Jamaican families, and to assess whether the instrument has construct and functional equivalence and is free of item or construct bias [44,45]. To the best of our knowledge, there have been no studies examining parental influences of adolescent sexual risk and no known measures of parent-child sexual communication validated for use in the Caribbean. Thus, the aims of this study were to: 1) describe patterns of mother-daughter sexual risk communication between urban Jamaican adolescent girls, ages 13 - 17, and their mothers; and 2) examine the psychometric properties of the PTSRC-III scale when used with urban Jamaican families.
2. METHODS
2.1. Study Design
The data were collected as part of a larger, randomized controlled trial study evaluating a theory-based, culturespecific HIV risk-reduction intervention for Jamaican adolescent girls, ages 13 - 17, and their mothers. Mother and daughter dyads were recruited into the trial and randomly assigned to participate in either an HIV risk-reduction intervention or a general health promotion intervention. The two groups were equivalent; there were no baseline differences between the control and intervention groups on demographic characteristics and main study variables [46].
All instruments and data collection procedures were pilot tested prior to their use in the main study. The 8-item PTSRC-III scale was included on the mothers’ and daughters’ pre-intervention baseline, 3-month follow-up and 6-month follow-up questionnaires. Baseline and 3-month follow-up data are reported here.
2.2. Procedure
The project was reviewed and approved by the New York University (NYU) University Committee on Activities Involving Human Subjects (UCAIHS) and the Ethics Committee of the Faculty of Medical Sciences, University of the West Indies (FMS/UWI) prior to participant recruitment and data collection. Prior to participation, mothers provided signed written informed consent for themselves and for their daughters, while daughters provided signed written informed assent in a separate room. After obtaining informed consent, data were collected by trained data collectors via paper-and-pencil questionnaires; because of literacy concerns, the questionnaires were also projected on the front wall of the room and read aloud during data collection. In addition, individual reading assistance was available and provided as needed in a discrete manner.
2.3. Sample
The sample consisted of 330 mother-daughter dyads from Kingston, St. Andrew and St. Catherine, Jamaica (urban parishes located on the southern coast of the island). Participants were recruited through community based organizations and via word-of-mouth referrals. In order to participate, daughters had to be between the ages of 13 and 17, unmarried, not currently pregnant, reside in one of the three parishes, and self-identify as Jamaican. Mothers had to be the primary female caregiver of the adolescent participant. In order to be eligible, both the mother and the daughter had to agree to participate.
2.4. Measures
The key outcome measure, the Parent-Teen Sexual Risk Communication (PTSRC-III) scale, consisted of 8 Likert-type items that asked about the amount of communication that occurred in each of eight sexual topic areas (birth control, sexually transmitted infections [STIs], preventing STIs, preventing HIV/AIDS, condom use, pressure to have sex, how to resist sexual pressure, postponing sex). Both mothers and daughters completed the PTSRC-III scale at each data collection point. Item wording was slightly different as appropriate for mothers (e.g., “How much have you told your daughter about…”) or daughters (e.g., “How much has your mother told you about…”). Response choices ranged from 1 - 5 (nothing [1], very little [2], some [3], a lot [4], and everything [5]). Possible scores ranged from 8 - 40 with higher scores representing more extensive sexual risk communication between the mother/ mother figure and daughter [24].
Other measures included daughters’ reports of age (in years), self-identified race/ethnicity, current school enrollment, living arrangements during the past year, condom use self-efficacy, and intentions to have sex in the next 3 months. Daughters also reported on their parents’ marital status, the type of relationship with the mother/ mother figure/female guardian (e.g., biological mother, grandmother, aunt, etc.), perceived closeness to mother, perceived importance of mothers’ opinions, and perceptions of mothers’ attitudes toward teen sex with a steady boyfriend. Measures assessed by mothers’ reports included mothers’ age (in years), education level, and current employment status.
2.5. Data Analysis
All analyses were conducted using Statistical Package for Social Sciences (SPSS) PASW version 18. Associations between continuous variables were assessed using Pearson’s product-moment coefficients (r), while those between categorical variables were calculated using Spearman’s rho (rs). All analyses utilized baseline data except where otherwise noted. Analyses that included data from the 3-month follow-up were limited to participants from the control group (n = 165) in order to avoid the potential confounding effects from participation in the HIV risk-reduction intervention. Although this decision reduced analytic power, the potential confound was seen as significant given that a major emphasis of the mothers’ HIV risk-reduction intervention curriculum was on increasing mother-daughter sexual communication. T-tests for differences in mean scores were conducted using dependent t-tests as mothers and daughters were not independent participants and comparisons of baseline and 3-month follow-up scores constituted repeated measures.
3. RESULTS
3.1. Participants
As is summarized in Table 1, daughters ranged in age from 13 and 17 years, with a mean age of 14.7 (1.3) years (n = 330). Almost all (97.3%) were currently enrolled in school. All self-identified as Jamaican (an inclusion criteria for the study). Most of the daughters (88.7%) reported living with the mother/mother figure all or most of the time; nearly 82% reporting being close or very close to their mother/mother figure. The mothers’ mean age was 39.8 (7.1) years (n = 330). Fewer than 15% of mothers were currently married to their daughter’s father; approximately 1/3 of mothers were employed full-time, while more than 1/3 were unemployed. The participant retention rate at 3-month follow-up was 96.5% [46].
3.2. PTSRC III Scale Scores
The Daughters’ baseline scores on the PTSRC-III scale extended across the full range of possible scores, 8 - 40, with a mean of 25.66 (9.14). As is shown in Table 2, scores varied across items. Daughters reported the greatest amount of sexual communication with mothers for Item 8 (communication about waiting to have sex) (mean = 4.02 [1.18]). In comparison, daughters reported the least amount of communication for Item 3 (com-


Table 1. Demographic characteristics of the sample.
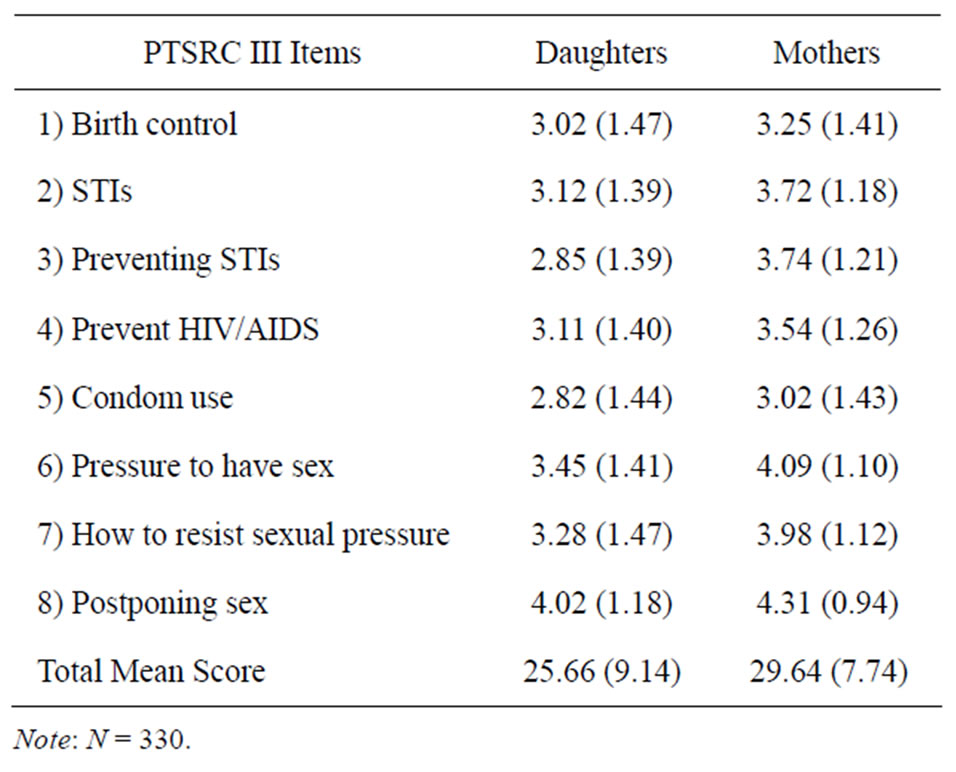
Table 2. PTSRC-III scale: mean item and total scores (baseline).
munication about preventing STIs) and Item 5 (communication about condoms) (means = 2.85 [1.39] and 2.82 [1.44], respectively).
Jamaican mothers’ baseline PTSRC-III scale scores also ranged from 8 - 40. Mothers reported slightly greater amounts of sexual communication, with a mean of 29.64 (7.74). Variation in mothers’ individual item scores was nearly identical to that for daughters. Mothers’ highest scores were for Item 8 (communication about waiting to have sex; mean = 4.31 [0.94]) and lowest scores were for Item 5 (communication about condoms; mean = 3.02 [1.43]). In contrast to daughters, mothers also reported low scores for Item 1 (communication about birth control; mean = 3.25 [1.14]).
Mean PTSRC-III scores at the 3-month follow-up were similar to those at baseline. The mean score for daughters was 26.47 (9.48). The mean score for mothers at 3-month follow-up was 31.98 (6.88). Sample sizes for these analyses were 160 and 165, respectively.
In terms of congruency in mothers’ and daughters’ reports of sexual communication, baseline reports showed moderate levels of agreement (r = 0.27, p < 0.001, n = 330), as did reports at the 3-month follow-up (r = 0.22, p < 0.001, n = 160). Mother-daughter differences in the baseline mean PTSRC-III scores were statistically significant (t = 7.07, df = 329, p < 0.001). Similarly, at the 3-month follow-up (n = 160), mothers’ PTSRC-III mean scores were significantly (t = 6.77, df = 159, p < 0.001) greater than those of their daughters.
3.3. Reliability
Cronbach’s alpha was computed to estimate the internal reliability of the 8-item PTSRC-III scale. Cronbach’s alpha coefficients for the daughters’ and mothers’ baseline scores were 0.93 and 0.92, respectively. Both Cronbach’s alphas were above the minimal acceptable value of 0.80 for well-designed scales [47,48]. These high Cronbach’s alphas indicated excellent internal consistency of the items when used with both Jamaican female adolescents and mothers. The inter-item correlation matrices showed that all items had positive and strong correlations, with correlation coefficients ranging between 0.51 - 0.80.
In addition to internal reliability, the stability or testretest reliability of PTSRC scores was assessed by examining the consistency of PTSRC-III scale scores between baseline and 3-month follow-up. As was previously discussed, these analyses were limited to data from control group participants in order to avoid confounding effects that participation in the mother-daughter HIV risk-reduction intervention might have on motherdaughter sexual risk communication. Daughters’ mean PTSRC-III scores at baseline and 3-month follow-up were 26.16 (8.69) and 26.47 (9.48), respectively. The two sets of scores were significantly correlated (r = 0.57, p < 0.001, n = 160); differences between the scores were not statistically significant (t = 0.47, df = 159, p = 0.64). Mothers’ PTSRC-III scores increased between baseline (29.96 [7.11] and 3-month follow-up (31.98 [6.88]). Mothers’ scores at the two time points were significantly correlated (r = 0.70, p < 0.001, n = 165); the differences between the two sets of mothers’ scores were significant (t = 4.74, df = 164, p < 0.001).
3.4. Factor Analysis
As is shown in Table 3, factor analysis for the 8-item PTSRC-III scale (using daughters’ reports) was undertaken using principal component analysis with confirmatory factor analysis [49]. The scree-plot, which shows eigenvalues in decreasing order, revealed one factor having an eigenvalue greater than 1, and a second factor with an eigenvalue just under 1. Factor 1, termed “Communication related to management or reduction of risk for adverse sexual outcomes” [24], included items 1, 2, 3, 4 and 5 and had an eigenvalue of 5.382. Factor 1 accounted for 67.3% of the variance. The only other meaningful factor included items 6, 7 and 8. This factor was previously labeled “Communication related to the prevention of sexual risk through prevention of sexual activity” [24]. This second factor had an eigenvalue of 0.626 and explained an additional 7.8% of the variance. The two factors were highly correlated (r = 0.717, p < 0.001); together they explained 75.1% of the variance.
3.5. Validity
Evidence of concurrent validity was found by examining the associations between daughters’ PTSRC-III scores and other variables that, based on the published literature, one would expect to be related to parent-teen sexual communication. As is shown in Table 4, daughters’ reports of PTSRC were significantly associated with

Table 3. Pattern matrix-principal component analysis.

Table 4. Bi-variate correlations between daughters’ reports of PTSRC and other variables.
mothers’ reports of PTSRC. Daughters’ PTSRC scores were also associated with daughters’ reports of comfort and ease with mother-daughter sexual communication, mother-daughter closeness, importance of mothers’ approval, and daughters’ perceptions that their mothers held more liberal attitudes towards teen sex with steady boyfriends. In addition, adolescent girls who reported greater amounts of PTSRC with mothers reported marginally greater condom use self-efficacy and marginally lower intentions to have sex in the next 3 months. Daughters’ ages were not associated with daughters’ PTSRC-III scores.
4. DISCUSSION
The current study findings demonstrated that the PTSRC-III scale performed well when used with urban Jamaican female adolescents and their mothers. Psychometric analyses found high levels of internal reliability, stability in reports across time, consistent two-factor structure, and associations with parent-child closeness, perceived importance of mothers’ opinions, and perceptions of mothers’ attitudes toward teen sex with a steady boyfriend. Marginal associations were also found between greater amounts of mother-daughter sexual communication and daughters’ reports of increased condom use self-efficacy and fewer intentions to engage in sex.
The findings of the current study were consistent with reports in the published literature. Jamaican female adolescents’ mean scores on sexual risk communication with their mothers were comparable to those reported for college students, late adolescent female drivers and African American college students in earlier US studies [24,31]. Mean PTSRC scores were 25.66 (9.14) in the current study, compared to 25.41 (8.55) for African American female late adolescent drivers [24], and 23.97 (9.43) for African American female college students [31]. Congruence between mothers’ and daughters’ reports of sexual communication was found to be moderate, with mothers reporting greater amounts of sexual communication than daughters; these findings were also consistent with the published literature [31,38,50].
The PTSRC-III demonstrated excellent internal reliability among Jamaican adolescent girls and mothers (α = 0.93 and 0.92, respectively). Inter-item correlations were all strongly and positively correlated with one another. The high level of internal consistency was similar to that found when the PTSRC-III scale was used in earlier studies with adolescent females in the US (α = 0.93 and 0.92) [24,31] and adolescents in Mexico (α = 0.94) [37,38]. Similar levels of internal reliability were also found when the instrument was used in South Africa (α = 0.92) (Hutchinson, M.K., personal communication).
Stability of PTSRC-III scores over time was also demonstrated. The test-retest correlations over a 3-month period were moderate to large and statistically significant for both daughters (r = 0.57, p < 0.001) and mothers (r = 0.70, p < 0.001). Although traditionally one aims for testretest reliability coefficients >0.80, the 3-month timeframe between the two measurement points was long [47, 48]. More importantly, because communication is not a time-invariant trait, one would expect some variation across time. Parent-teen sexual communication would be expected to change, ebb and flow, as the adolescent grows and develops and her social situation, dating and/or sexual behaviors change. As the PTSRC scale questioned respondents about total amounts of informational sexual exchange, one would expect that scores would increase over time.
The factor structure for the PTSRC-III scale was the one area in which minor differences were found between the current study’s findings in Jamaica and previous US studies. As was reported, the factor analysis found two factors. One factor loaded with an eigenvalue greater than 1.0. This factor had a very similar loading pattern, comparable eigenvalue and explanation of variance as in the initial psychometric testing of the PTSRC-III instrument [24]. Although the second factor in this study did not have an eigenvalue greater than 1.0; the loading pattern and explanation of variance were very similar to the factor 2 described in the initial psychometric testing of the PTSRC-III instrument [24]. As in the initial assessment of the instrument, the two factors were highly correlated (r > 0.65).
5. CONCLUSION
Instruments developed and tested in one culture may not produce dependable results when used in different cultures. The cross-cultural validity and reliability of instruments must be evaluated before researchers may be confident that the obtained scores are accurate and reliable representations of the construct in the new cultural context [44,45,51]. The PTSRC-III scale has been found to be both valid and reliable for use in Jamaica and able to produce consistent results across cultures. The crosscultural applicability of the instrument allows for international comparisons.
6. ACKNOWLEDGEMENTS
This research was funded by a grant from the National Institutes of Health/National Institute of Nursing Research (R01 NR010478; M.K. Hutchinson, PI).