Accessory breast poorly differentiated adenocarcinoma with positive HER2 gene amplification: A case report ()
2. CASE REPORT
This 56 year post menopausal Malaysian lady of Indian ethnicity initially presented to a private institution for a painful axillary swelling that has been present for the past 6 months. This lady attained puberty at the age of 15 and she became menopausal 11 years ago. She has 4 children, who were all breast fed. She has never consumed oral contraceptives neither has she been on hormone replacement therapy. Her co-morbids include Mellitus and Bronchial Asthma.
On examination of the axillary during her visit to the private institution, they found a mass measuring 5 × 6 cm with no overlying skin changes. A bilateral mammogram was done which revealed a BIRADS 2 lesion of the ipsilateral breast suggestive of a fibroadenoma.
Therefore it was decided to proceed with an incisional biopsy. The histopathology was reported as containing malignant large cell tumour infiltrates (Figure 1) in favour of a metastatic poorly differentiated adenocarcinoma.
Subsequently referred to the General Hospital, where a Computer Tomography Scan of the Head Neck, and Thorax was done which revealed multiple cervical and axillary lymphadenopathy without a significant primary lesion. In view of the histopathological findings being in favour of a metastatic poorly differentiated adenocarcinoma, we proceeded with an OGDS and Colonoscopy to further investigate for a primary lesion only to reveal normal investigative findings.
Finally it was decided to proceed with a PET-scan (Figure 2), which showed multiple FDG-avid left axillary lesions suspicious of metastatic lymph node disease and the primary lesion indeterminate.
Consequently an excision biopsy of the axillary mass was done, histopathologically reported as a poorly differrentiated adenocarcinoma with positive HER2 gene amplification.
She was consequently referred to the oncologist for adjuvant chemotherapy, which she responded well to.
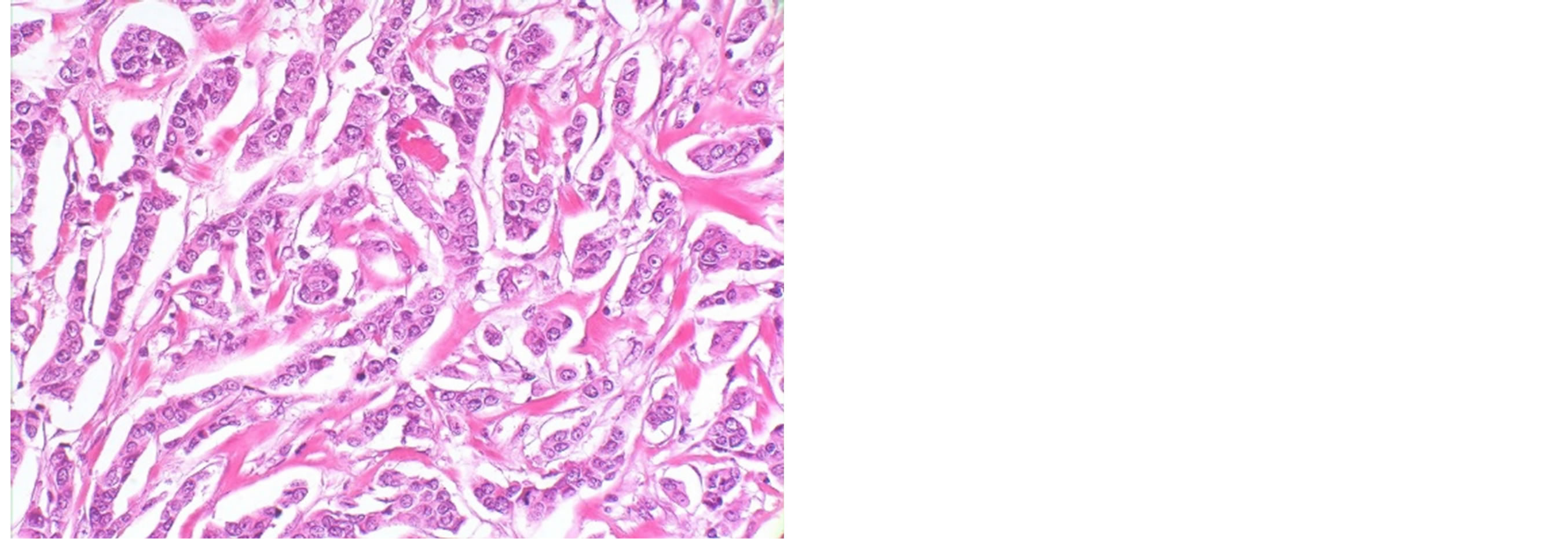
Figure 1. Malignant large cell tumourinfiltrates under 100 nm magnification.
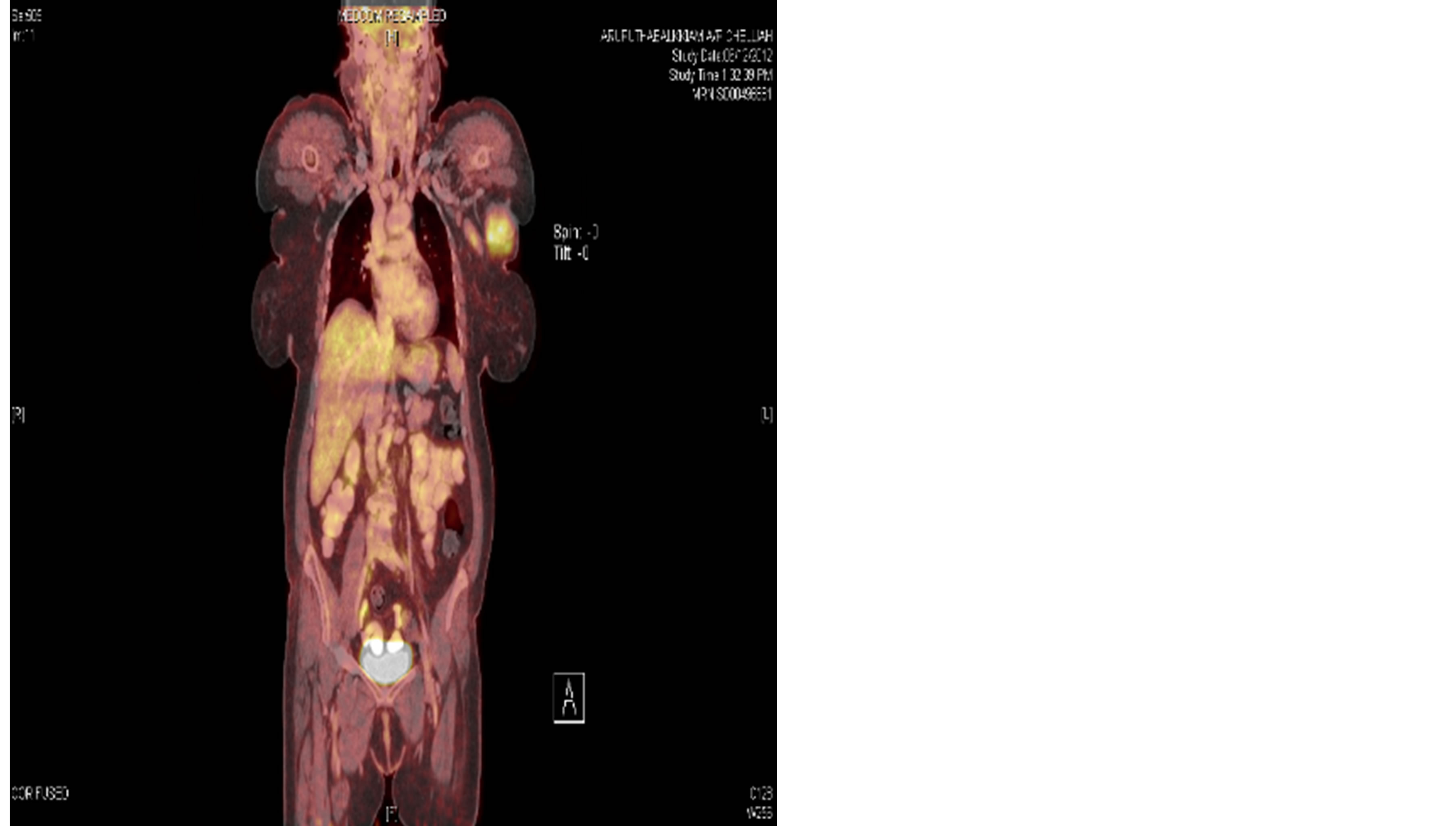
Figure 2. PET-scan revealing multiple FDG-avid left axillary lesions suspicious of metastatic lymph node disease.
3. DISCUSSION
Accessory breast tissue occurs in 2 - 6 percent of the general population [4] and the occurrence of a primary malignancy arising from this tissue is rare [1]. This accessory breast is the consequence of partial regression of the primitive milk streak that develops in the embryo [5], the commonest location being the axilla [4]. Being breast tissue, it is physiologically susceptible to homeostatic hormonal controls [6] and tends to develop during puberty and become apparent during pregnancy [5].
These accessory breasts associated with pathological changes such as mastitis, fibroadenoma, cystosarcoma, carcinoma, and duct hyperplasia have been reported, as described by Goyal S. et al. [4]. Primary accessory breast cancer is a rare form of breast cancer, in which this case reports a poorly differentiated adenocarcinoma with positive HER2 gene amplification.
Devine et al. describes that the most common morphological variant is that of the invasive ductal carcinoma type.
The overall prognosis is basically similar to that of breast cancer. Giron G. et al. mentions that the likelihood of an accessory breast malignancy being metastatic is much higher, being in close proximity with the axillary lymph node basin [7] hence the findings of multiple cervical and axillary lymphadenopathy described in this case.
Some authors recommended radical ipsilateral mastectomy if regional lymph nodes are involved, however Evans and Guyton [8,9] have concluded that ipsilateral mastectomy in addition to axillary lymph node dissection was not superior to local excision with node dissection.
This case was consequently referred to the oncologist for adjuvant chemotherapy and also referred to Breast and Endocrine Unit for opinion on a Mastectomy on the ipsilateral side. The Breast and Endocrine unit concluded that there was no need for a mastectomy as the PET-scan did not show any disease arising from the breast.
It is stated that tumours with HER2 gene amplification respond well to trastuzumab (Herceptin) and taxanechemotherapy, with the standard duration of treatment being one year [8,10]. But latest trials [9,10] have proven the efficacy of T-DM1 (ado-trastuzumabemtansine; Kadcyla) in the treatment of metastatic breast cancers with HER2 gene amplification.
4. CONCLUSION
Overall prognosis is similar to that of a carcinoma of the normal breast, therefore early diagnosis is imperative to ascertain curable status and improve prognosis. Triple assessment is vital in any breast cancer for accurate diagnosis of any patients presenting with an axillary swelling.
CONSENT
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
COMPETING INTERESTS
The authors declare that they have no competing interests.
AUTHORS’ CONTRIBUTIONS
DFB drafted the manuscript. RT was clinically responsible for the patient’s care. JSK was responsible for pathology.
NOTES
#Corresponding author.