Profile of Amputations in National Orthopaedic Hospital, Dala, Kano ()
1. Introduction
Amputation is the removal of a part of a body through a bone while disarticulation is the removal of a part through a joint. It is a common procedure undertaken by surgeons worldwide. There were about 1.6 million amputees in 2005 in the United State of America, and the reasons range from a dead body part, a dangerous body part or nuisance from a body part. This can be further broken into individual causes such as trauma, vascular injuries, infections, neoplasia etc. [1] [2] .
The reasons for the amputations also vary in different parts of the world and also among different regions of same nation and this may be due to some cultural practices or prevalent disease conditions [3] .
We therefore undertake to study the profile of amputations in our centre Visa-Vis amputations, the parts affected, duration of hospital stay as well as the morbidity suffered from the procedure.
Indications of amputation:
1) Loss of viability secondary to reconstructive ischemia 2) Trauma 3) Tumour 4) Extensive infection which does not respond to conservative measures Two third of amputations in the western societies are due to peripheral vascular diseases and commonly are the above knee and below knee amputations [4] .
At each level, the operative procedure and post operative management are directed at achieving primary healing a painless stump that will withstand the pressure of prosthesis and relatively unrestricted for ambulation.
Selection of level: Several factors attributed to the selection of levels of amputation which includes the indication, available stump, prosthesis fixation and cosmetics required. In tumours, wide local excision is done while in peripheral vascular diseases the extend of healthy tissues are considered.
Above Knee Amputation (AKA) expends about energy to ambulate compared to Below Knee Amputation (BKA), while the overall mortality for amputations performed for isolated tumours, traumas or infections were less than 3% [5]
Extremity re-plantation: successful hand re-implantation was registered in 1963. Microvascular techniques result in increasing success. A summary of the experiences from China, US and Switzerland showed that one third had functional recovery and one third was fair to poor results [6] .
Studies showed that up to four percent of good function follows above elbow amputation, proximal forearm had 0% - 70%, while distal forearm recorded 50% - 83%, wrist in 25% - 80%, palm was seen in 25% - 70%, thumb had 32% - 90%, while proximal PIP joint was seen in 70% and distal to PIP was recorded in 100% [1] [4] .
Guillotine injuries have higher degree of success at re-implantation compared to crush injuries. Also if duration of anoxia is less than 20 hours, the success rate is higher [4] [5] .
The essential structures of the dismembered extremity must be intact and the severed limb reasonably well preserved if re-implantation is attempted [5] .
2. Materials and Method
The case files of all patients who had amputations in the National Orthopeadic Hospital Dala, Kano Nigeria between 1998-2012 were retrospectively analyzed. After a literature search was done a proforma was designed to extract the discrete and non discrete information of the patients in the case folders. Data on age, sex, intra-operative diagnosis, part amputated, duration of hospital stay and the morbidity suffered in the course of treatment were analyzed, and the results were compared with other studies. Ethical clearance was obtained from the hospital research and ethics committee and there was no research grant obtained for this study.
3. Results
A total of 196 patients were studied, including 159 males and 37 females with a male to female ratio of 4.3:1. Their age ranged from 5 years to 67 years with the median age of 36 years.
4. Discussion
Amputation is the removal of a body part through a bone is a common orthopaedic procedure with different outcome depending on the indication, presentation and the type of amputation done.
In our study, we found a total of 196 cases who had amputation in our centre within the period of 15 years. Out of which, 159 (81.12%) were males and 37 (18.88%) were females with a male to female ratio of 4.3:1 which differs from findings by Lcle, A. et al., Chalya, P.L. et al., Dos Santos Taveres, D.M. and Enweluzo, G.O. who discovered a male to female ratio of 1.2 - 1.7:1 in different centres across the world [7] -[10] (Figure 1).
We found a mean age of 35 years which is slightly higher than the findings by Chalya PL in Costa Rica, who found a mean of 54.2 years and Enweluzo, G.O. in Lagos who found a mean age of 43 years [6] [9] .
68 (31.69%) out of 196 patients had below knee amputations followed by 54 (27.55%) patients who had above knee amputations, while 27 (13.78%) had above elbow amputations. This compares favourably with the findings by Lacle, A., Chalya, P.L. & Enweluzo, G.O. [6] [7] [9] (Figure 2).
Also we discovered that 66 patients had left sided lower limb amputations followed by 53 patients who had had right sided upper limb amputations; and only 3 patients had a bilateral amputations; and previous writings studied were silent on side affected.
In addition, we also discovered that most of our cases were secondary to traditional bone setters splintage (tight occlusions of the blood supply by traditional splints leading to gangrene) accounting for 71 cases (36.22%) followed by road traffic accidents in 36 cases (18.37%) and the others. This is contrary to the findings by Lacle A. & Enweluzo who found diabetic foot to be the commonest cause and Fagundes who found vascular injury to be the commonest cause [6] [7] [11] .
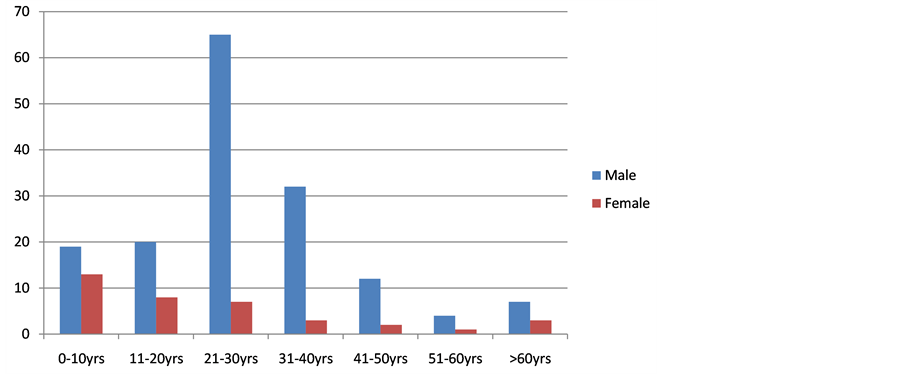
Figure 1. Histographic presentation of age distribution.
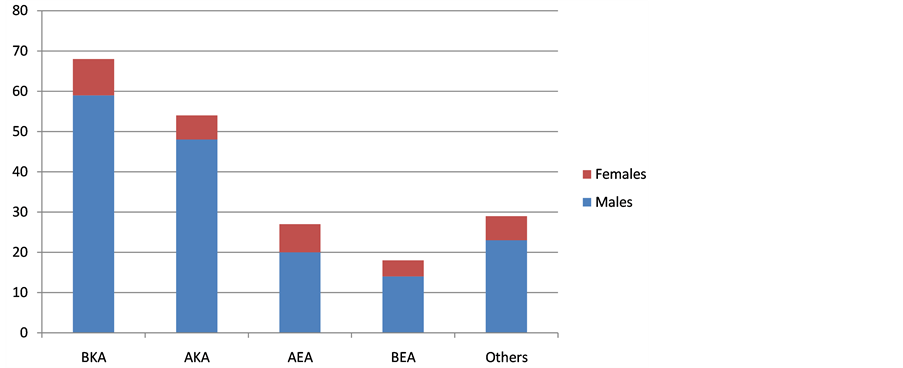
Figure 2. Shows distribution of their level of amputation: Below Knee Amputation (BKA), Above Knee Amputation (AKA), Above Elbow Amputation (AEA), Below Elbow Amputation (BEA).
The range of hospital stay was between 5 days to 7 months with an average of 30 days in most patients and this differs from the findings by Chaya, P.L. who discovered a range of 18 - 28 days with an average of 36.24 days [7] (Figure 3).
158 (80.61%) out of 196 patients who had amputations within the period were discharged and only 3 (1.53%) suffered some morbidity with only 1 (0.51%) mortality while the remaining were either referred in the course of treatment or discharged themselves against medical advice which is contrary to the findings by Chalya, P.L. who found a mortality rate of 1.325 and Enweluzo, G.O. who found a mortality rate of 11.8% [7] [9] (Figure 4).
5. Conclusions
Above findings have indicated that most of our cases were males with a mean age of 35 years and most patients had a below knee amputations in most instances left sided which may be explained by left sided driving instead of right sided steering in other communities.
Most cases suffered a secondary excessive occlusion of the vascular supply leading to gangrene and ultimate amputation and this is avoidable through massive public enlightment campaign.
In Africa and other part of the developing world, the problem of Traditional Bone Setters (TBA) intervention is serious one which needs an urgent attention by the authorities.

Figure 3. It shows distribution by hospital stay.

Figure 4. It shows distribution by outcome.
Completing Interest
The authors declare that they have no completing interests.
Perspective
To see how we can reduce hospital stay and reduce the avoidable amputations from Traditional Bone Setters (TBS) by:
• Doing primary amputations at appropriate levels
• Ensuring aggressive debridement and wound care
• Using the appropriate antimicrobial agents
• Prompt rehabilitation
Authors Contributions
Dr. Mamuda, A.A. carried out: conception of the paper, drafting of manuscript, design of the study, analysis of data and interpretation of data and revising the manuscript.
Dr. Salihu, N.M. carried out: drafting of manuscript, acquisition of data, analysis and interpretation of data.
Dr. Abubakar, M.K. carried out: acquisition of data, design of study and revising the manuscript.
Dr. Kabir, M.A. carried out: drafting of manuscript, conception and design of study and revising the manuscript.
Dr. Mustapha, I. carried out data acquisition, revising the manuscript and analysis of data.
Dr. Ujudud, M.M. carried out drafting of manuscript, design of study, acquisition of data, analysis and interpretation of data and revising the manuscript.
NOTES
*Corresponding author.